Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send washington claim form pdf via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out wa claim form with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
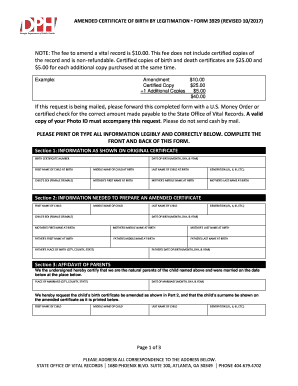
Click ‘Get Form’ to open the wa claim form in the editor.
Begin by entering your personal information in the designated fields, including your name, date of birth, and contact details. Ensure all entries are clear and legible.
Provide details about the incident that led to your claim. This includes the date, time, and location of the event. Be specific to help streamline processing.
List all witnesses and involved parties in the appropriate sections. Include their contact information for verification purposes.
Attach any supporting documents such as medical records or photographs that substantiate your claim. Use our platform's upload feature for convenience.
Review all entered information for accuracy before signing the form electronically. Ensure you have checked all required boxes.
Once completed, submit your form directly through our platform or print it out for mailing to the Office of Risk Management.
Start filling out your wa claim form today using our platform for a seamless experience!
Filing a Claim - Risk Services - University of Washington
If you would like to file a claim regarding an incident other than a vehicle accident, please complete the UW Liability Claim Form. In addition to one of theRead more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.