Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send health insurance marketplace statement via email, link, or fax. You can also download it, export it or print it out.
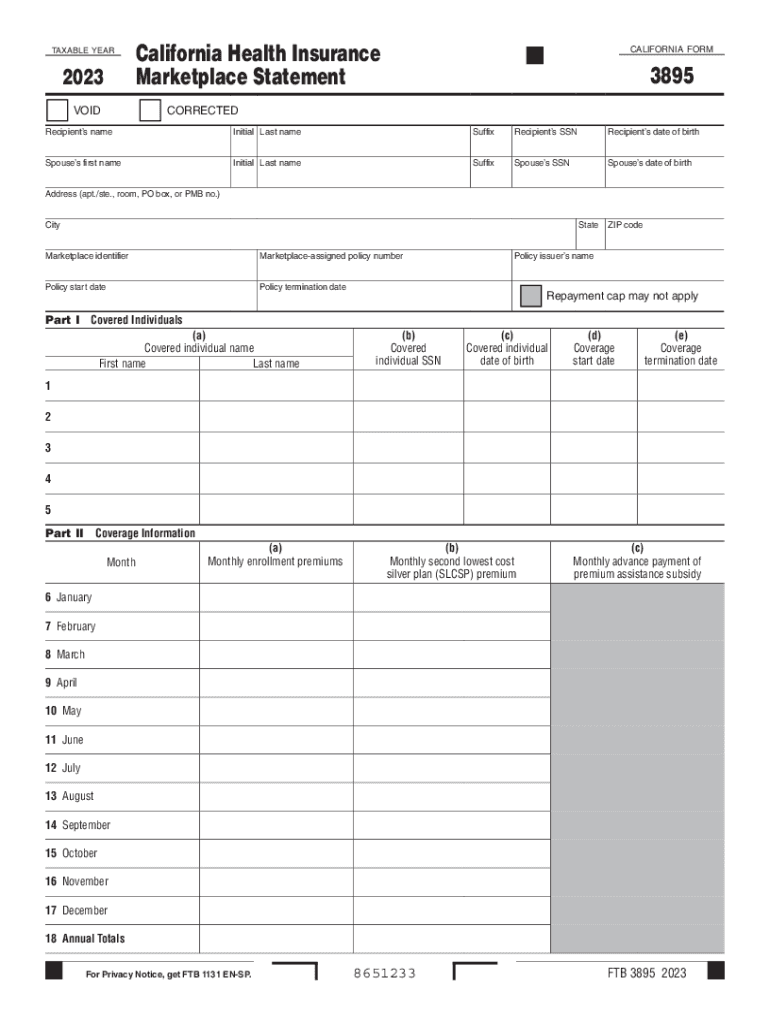
How to use or fill out 2023 Form 3895 California Health Insurance Marketplace Statement with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
Click ‘Get Form’ to open the 2023 Form 3895 in the editor.
Begin by entering the recipient’s name, Social Security Number (SSN), and date of birth in the designated fields. Ensure accuracy as this information is crucial for identification.
Next, input your spouse’s details if applicable, including their name, SSN, and date of birth. This section is important for joint coverage.
Fill in your address information accurately, including city, state, and ZIP code. This helps in proper documentation and correspondence.
In Part I, list all covered individuals by entering their names, SSNs, dates of birth, coverage start dates, and termination dates as necessary.
Proceed to Part II where you will enter monthly enrollment premiums and other relevant financial details for each month of the year.
Review all entered information for accuracy before finalizing your form. Use our platform's features to make any necessary edits easily.
Start using our platform today to fill out your forms online for free!
Fill out 2023 Form 3895 California Health Insurance Marketplace Statement 2023 Form 3895 California Health In online It's free
See more 2023 Form 3895 California Health Insurance Marketplace Statement 2023 Form 3895 California Health In versions
We've got more versions of the 2023 Form 3895 California Health Insurance Marketplace Statement 2023 Form 3895 California Health In form. Select the right 2023 Form 3895 California Health Insurance Marketplace Statement 2023 Form 3895 California Health In version from the list and start editing it straight away!
What is the form FTB 3895 California Health Insurance Marketplace statement?
Form FTB 3895 is used to report certain information to the Franchise Tax Board (FTB) about individuals who enroll in a qualified health plan through the California Health Insurance Marketplace (Marketplace). The term Marketplace refers to the California state Marketplace, also known as Covered California.
What is a 1095-A-3895 form?
The forms IRS Form 1095-A and FTB 3895 are important forms that you will need to process (or provide to your tax preparer) when filing taxes if you had health insurance on the marketplace and received subsidies.
What is covered in California 1095-A?
The 1095-A Form is a Covered California statement that is needed to file your Federal Income Tax Return. It shows how many months you had health insurance and how much Advanced Premium Tax Credit (APTC) you received.
How do I get my 1095 marketplace statement from health insurance?
How do I get my 1095-A Form? Members of Covered CA can access their 1095-A Forms via mail or through a secure online portal, depending on their chosen method of communication with Covered CA. If email is the selected mode, its crucial to anticipate an email notification from Covered CA towards Januarys end.
How do I get a copy of my Covered California 3895 form?
If a consumers communication preference is mail, they will receive their Form FTB 3895 in the mail. All consumers can access their Form FTB 3895 in their CalHEERS account home page, or under Documents Correspondence, even if their preference is mail.
ftb 3895
How to get 3895 Form from Covered Californiais form 3895 the same as 1095-aForm 3895 for 2024did you have health insurance from the covered california marketplace (coveredca.com) (form 3895)?Covered California loginForm 3895 RedditHow to get Form 3895Do i need Form 3895 to file taxes
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
A guide for high deductible health plans | Cardinal at Work
Oct 18, 2023 This page will help you discover how an HDHP works, the benefits of an HSA, and how to maximize the HSA to build short-term and long-term savings.
2023 Form 3895 California Health Insurance Marketplace
2023. California Health Insurance. Marketplace Statement. CALIFORNIA FORM. 3895. VOID. CORRECTED. Recipients name. Initial Last name. Suffix. Recipients SSN.
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.