Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send dd form 2870 via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out dd form 2870 with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
Click ‘Get Form’ to open the dd form 2870 in the editor.
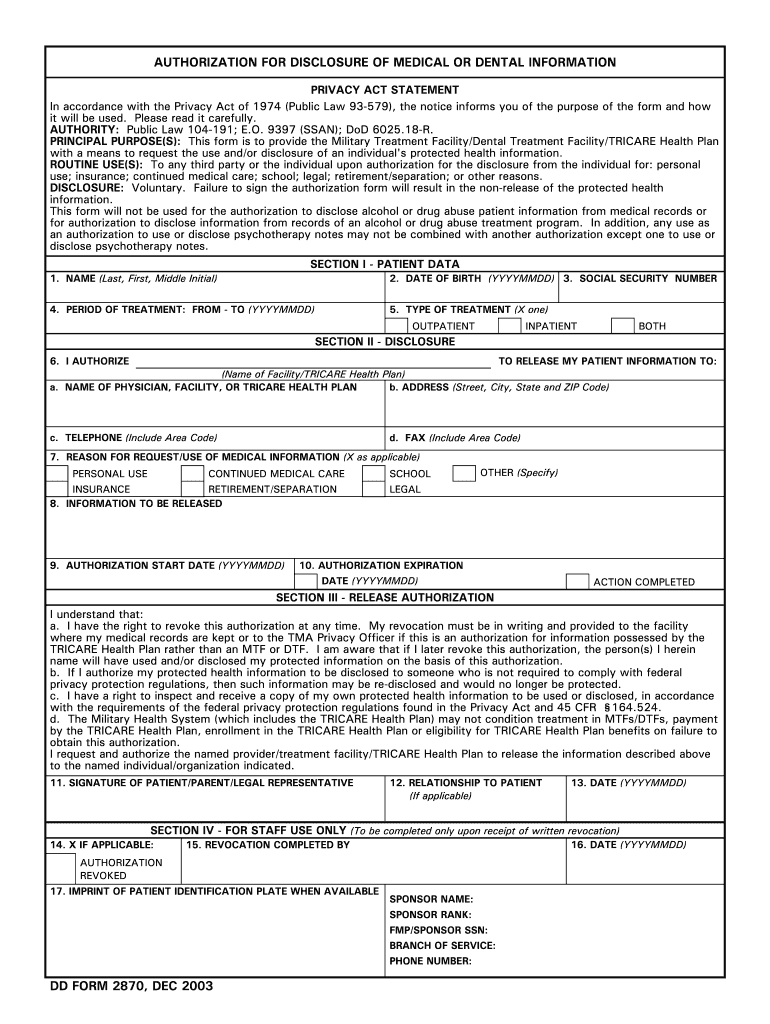
Begin by filling out Section I - Patient Data. Enter your full name, date of birth, and social security number accurately.
Indicate the period of treatment by specifying the start and end dates in YYYYMMDD format. Select the type of treatment you received: Outpatient, Inpatient, or Both.
In Section II - Disclosure, provide the name and address of the facility or TRICARE Health Plan to which you are authorizing disclosure. Include a contact telephone number and fax number if applicable.
Select the reason for requesting your medical information from the options provided, such as personal use or continued medical care.
Complete Section III by signing and dating the form. Ensure that you understand your rights regarding this authorization.
Start using our platform today to fill out your dd form 2870 online for free!
It is important for service members to keep their DD Form 93 updated to ensure benefits docHub the intended beneficiaries in a timely fashion. To update your form, call or visit your personnel center.
What is dd form 2870 used for?
AUTHORITY: Public Law 104-191; E.O. 9397 (SSAN); DoD 6025.18-R. PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individuals protected health information.
What is the purpose of the authorization to release information?
Key takeaways. A HIPAA authorization form authorizes the release of your protected health information (PHI) to certain individuals and allows them to speak with medical providers about your health care.
What is a 2870?
Authorization for Disclosure of Medical or Dental Information (DD Form 2870) Your provider or contractor will use this form to get your permission to share your protected health information to a third party for personal use; insurance; continued medical care; school; legal; retirement or separation; or other reasons.
What is the DD Form 1750 packing list?
The DD Form 1750 is a packing list form used by the Department of Defense. It serves several important purposes: To list all items packed for transport. To document the quantity and condition of items.
2003 dd 2870
Dd form 2870 pdfPrintable dd form 2870DD Form 2870 PDF download freePrintable DD form 2870 downloadDD Form 2870 army pubsDd form 2870 2024DD Form 2870 TRICAREDD Form 2870, NOV 2023
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
What is the purpose of the notice of privacy practices?
A consent to release medical information form will typically be requested when someone wants a copy of their own medical records or would like to have them sent to a third party. The request is made to the healthcare provider, therapist, or organization that has the patients records.
disclosure authorization form
DD Form 2870, Authorization for Disclosure of Medical or
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/Read more
Laboratory, Field, and Analytical Procedures for Using
To reduce or eliminate the human and ecological health risks manifested by these sediments, federal, state, local, and tribal regulatory authorities have aRead more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.