georgia first report of injury
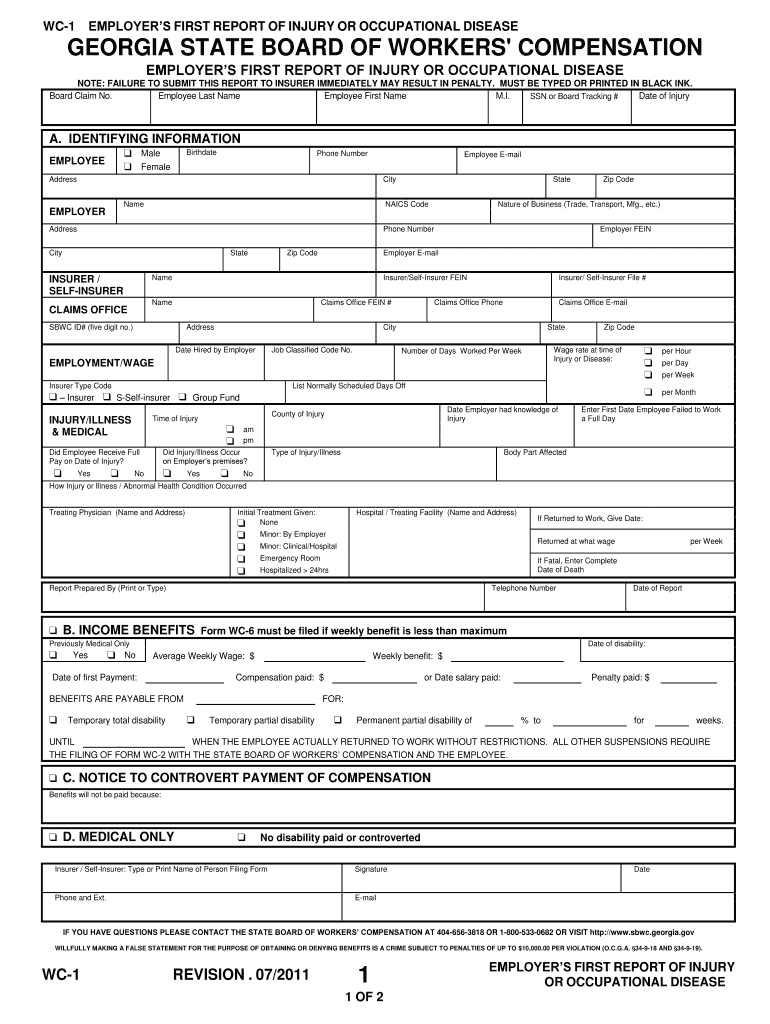
wc-1 - employers first report of injury or occupational disease
Complete Section A of this form immediately upon your knowledge of an injury and send the WC-1 to your insurance company or self-insurer claims office. FAILURERead more
Learn more
NEW YORK STATE MEDICAID PROGRAM DURABLE
Jul 19, 2005 Leave this box blank if condition is related to an auto accident other than no-fault or if no-fault benefits are exhausted. Other Liability.Read more
Learn more
EMPLOYERS FIRST REPORT OF INJURY OR
Report serious injuries immediately by telephone to your insurers claims department, then file this form with your insurance company or self-insurer claimsRead more
Learn more