bcbs reimbursement form
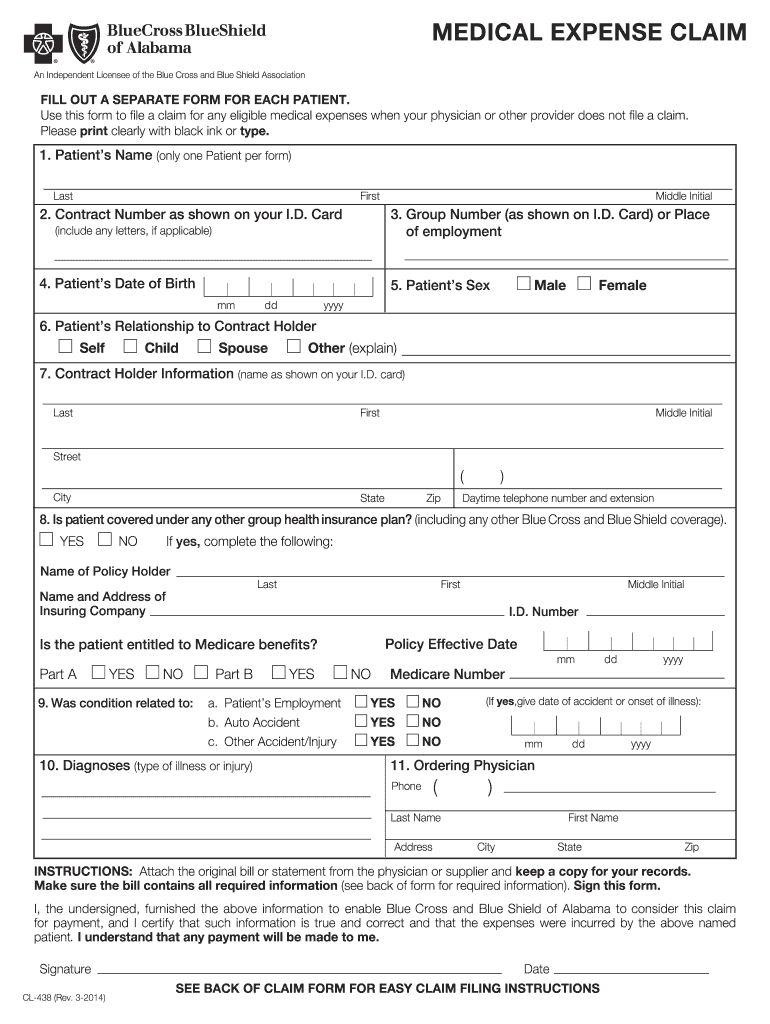
MEDICAL EXPENSE CLAIM
Sign this form. I, the undersigned, furnished the above information to enable Blue Cross and Blue Shield of Alabama to consider this claim for payment, andRead more
Learn more
Authorization for Disclosure of Protected Health Information
This authorization will permit Blue Cross and Blue Shield of Alabama and its business associate(s) on behalf of your Health Plan to disclose your healthRead more
Learn more
Parts Manual RTC50G08-20
Fill out the Warranty RegistrationForm in full and return it to within 30 Days. Make certain the Serial Number of the Machine is recorded on theWarranty CardRead more
Learn more