01. Edit your pfizer enrollment form for group a medicines online
Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send it via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out Pfizer Patient Forms with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
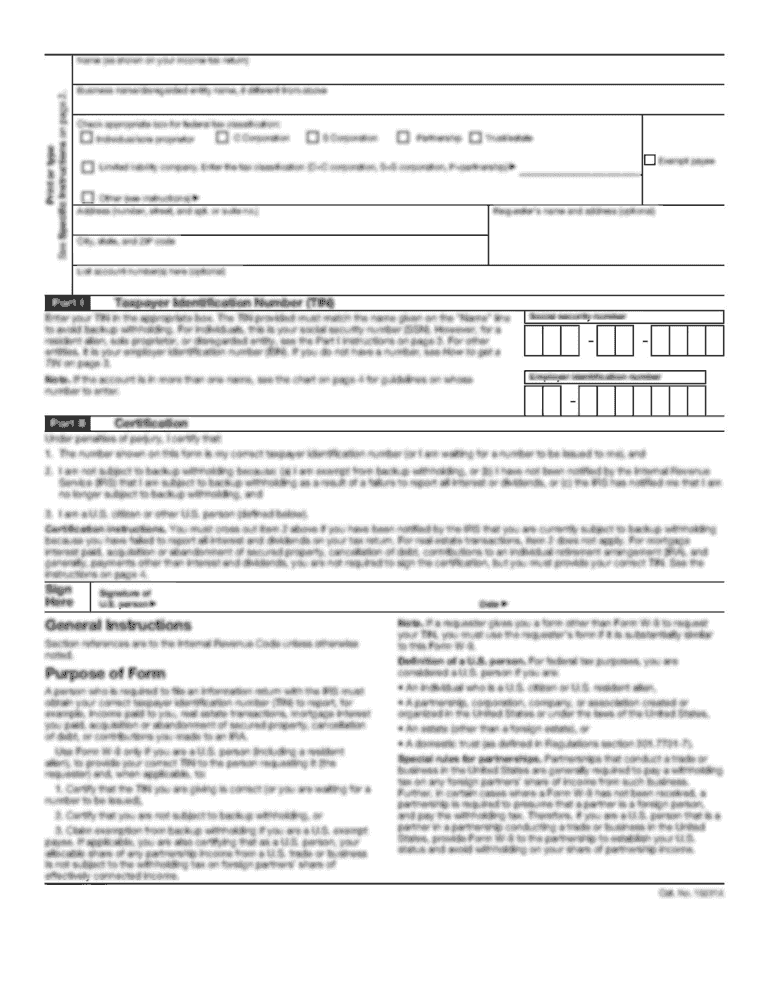
Click ‘Get Form’ to open the Pfizer RxPathways enrollment form in the editor.
Begin by filling out the patient information section. Provide your name, address, date of birth, and total annual income. Ensure you have documentation ready to support your financial claims.
In the prescription coverage section, indicate whether you have insurance. If yes, provide details about your coverage type and policy information.
Sign the patient privacy and consent section at the bottom of page 3, affirming that all provided information is accurate.
Next, ask your prescriber to complete their section on page 4. They will need to provide their details and sign off on the prescription order.
Gather all required documents including proof of income and any necessary prescriptions. Make photocopies for your records as these documents typically will not be returned.
Finally, submit your completed form either by mailing it to Pfizer RxPathways or having your prescriber fax it directly.
Start using our platform today for free to simplify your Pfizer patient forms process!
Who is eligible for Pfizer patient assistance program?
In order to be considered for the Pfizer Patient Assistance Program, you must: Be uninsured or government insured and unable to afford your co-payment. Government insurance includes, but is not limited to, Medicare, Medicaid, Champus/TRICARE and VA.
What is the PAP patient assistance program?
Patient Assistance Program (PAP) a program in which pharmaceutical manufacturers provide financial or medication assistance (pharmaceuticals) to low- income individuals.
What is the income limit for AZ and ME patient assistance?
You may be eligible if you meet the following criteria: 1. You have an annual household income* at or below: $35,000 for a single person $48,000 for a family of two $60,000 for a family of three $70,000 for a family of four $80,000 for a family of five * Income limits may be higher in Alaska and Hawaii.
What is the Bumex patient assistance program?
Patient Advocate Foundations Co-Pay Relief program exists to help reduce the financial distress you or your family may face when paying for your BUMEX treatment. If you qualify and can demonstrate the need, the foundation will provide you with direct payment covering co-pays, co-insurance, and deductibles.
What is the income limit for Novo Nordisk patient assistance program?
Who is eligible for this program? Patients must be a US citizen or legal resident, must have a total household income at or below 400% of the federal poverty level, and must be uninsured or have Medicare. Note: Patients with private or commercial insurance are not eligible for the PAP.
Related Searches
Pfizer dermatology Patient portalPfizer Patient portalCIBINQO enrollment form pdfLITFULO enrollment form PDFPfizer Patient Assistance Program application PDFCIBINQO enrollment form 2026LITFULO enrollment form 2026LITFULO Patient Assistance application
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
Pharmaceutical manufacturers may sponsor patient assistance programs (PAPs) that provide financial assistance or drug free product (through in-kind product donations) to low income individuals to augment any existing prescription drug coverage.
What is the Zirabev patient assistance program?
With this program, eligible patients may pay as little as $0 co-pay per ZIRABEV treatment, subject to a maximum benefit of $25,000 per calendar year for out-of-pocket expenses for ZIRABEV including co-pays or coinsurances. The amount of any benefit is the difference between your co-pay and $0.
Related links
Consent for Pfizer-BioNTech Covid-19 Immunization
For patients to be vaccinated. The following questions will help us determine if there is any reason we should not give you Pfizer/BioNTech COVID-19.Read more
Send us your original prescription form, completed and signed application form, and copies of your proof of income. If approved, well send up to a three-monthRead more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.