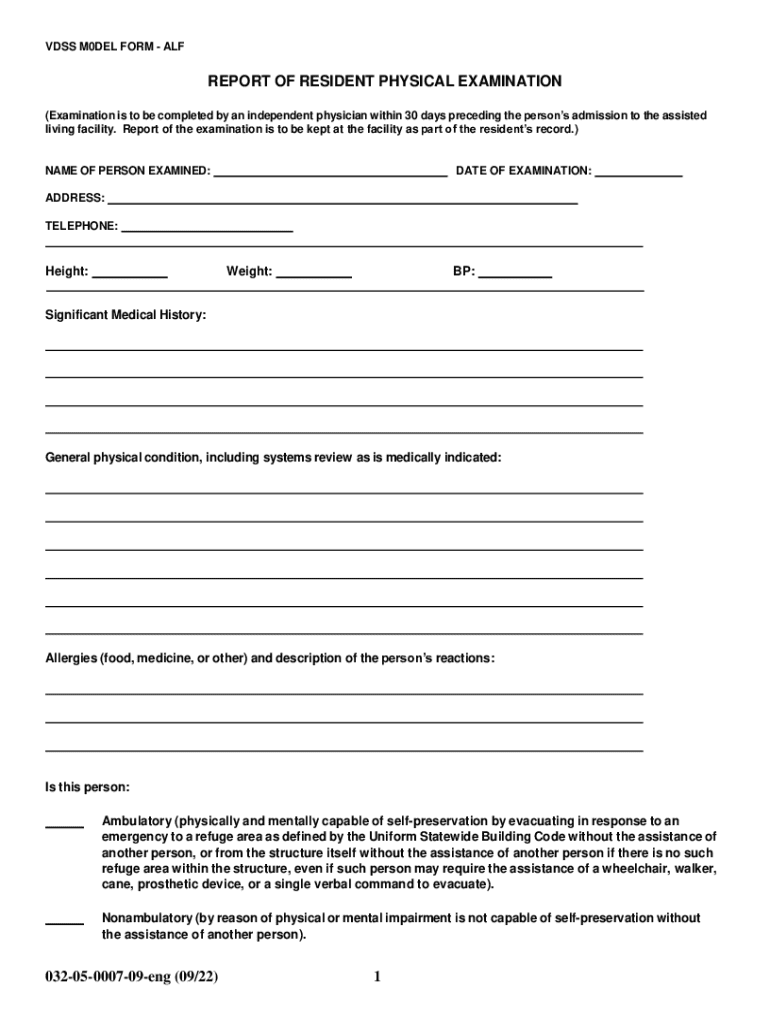
Definition and Overview of the Report of Resident Physical Examination
The Report of Resident Physical Examination is a comprehensive document intended for residents entering assisted living facilities. It is instrumental in outlining a resident’s physical health status, ensuring that they receive the appropriate care and support upon admission. This document covers various aspects such as personal information, medical history, physical condition, and specific care needs. By providing a detailed evaluation, the form assists healthcare providers and administrators in crafting individualized care plans to enhance the resident’s living experience.
How to Use the Report of Resident Physical Examination
Using the Report of Resident Physical Examination involves a systematic process aimed at accurately capturing a resident's health status. This form is generally filled out by healthcare professionals who conduct a thorough physical examination. Key areas assessed include:
- Personal Information: Collect basic data such as the resident’s name, birth date, and emergency contacts.
- Medical History: Document past and present health conditions, hospitalizations, surgeries, and chronic diseases.
- Physical Condition: Evaluate vital signs, organ functionality, and mobility status to determine the resident's health baselines.
The completed report is then reviewed by the facility’s healthcare team to plan any necessary medical interventions or adjustments to the resident’s daily routine.
Steps to Complete the Report of Resident Physical Examination
Completion of the Report of Resident Physical Examination requires adherence to a structured sequence of actions to ensure accuracy and completeness:
- Gather Personal Information: Begin by accurately recording the resident’s personal details.
- Conduct a Thorough Medical Review: Evaluate medical history by consulting previous records and interviewing the resident or their family.
- Perform a Detailed Physical Examination: Check vital signs and assess each bodily system for indicators of health concerns.
- Assess Tuberculosis Risk: Follow specific guidelines to screen for TB, in line with Virginia Department of Health protocols.
- Compile the Report: Ensure that every section is duly filled out with precise information, indicating any required follow-up actions or special care requirements.
Healthcare professionals should ensure that all data is captured accurately to aid the development of tailored medical and nutritional plans for the resident.
State-Specific Rules for the Report of Resident Physical Examination
Rules governing the Report of Resident Physical Examination can vary by state, which underscores the importance of understanding local regulations. In Virginia, for example, there are specific directives for tuberculosis screening and risk assessment. Healthcare providers must follow state guidelines carefully, as they impact both the examination process and the subsequent care plan development. This ensures regulatory compliance and enhances the safety and well-being of residents within these facilities.
Key Elements of the Report of Resident Physical Examination
Several critical elements make up the Report of Resident Physical Examination, thereby ensuring a comprehensive review of an individual’s health:
- Vital Signs: Record information such as temperature, blood pressure, and heart rate.
- Functional Status: Evaluate the resident’s ability to perform daily activities and any need for assistance.
- Medication Management: Detail current medications, dosages, and any allergies that factor into their treatment protocols.
- Special Care Needs: Identify any specific requirements for ongoing medical or custodial care.
These components collectively provide a holistic view of the resident’s well-being, informing the care strategy that will be implemented.
Who Typically Uses the Report of Resident Physical Examination
The Report of Resident Physical Examination is primarily utilized by healthcare professionals in assisted living facilities. Physicians, nurses, and medical assistants use the form to assess incoming residents’ health conditions. Facility administrators also rely on it to ensure they provide adequate resources and staff to address the diverse needs of each resident. Additionally, family members of residents may review this report to remain informed about their loved one’s health status and care plan.
Legal Use of the Report of Resident Physical Examination
Legally, the Report of Resident Physical Examination serves as a critical document in complying with state health regulations and facility admission requirements. It provides a certified medical evaluation that establishes the resident's fitness for the living arrangement and identifies any necessary accommodations. Keeping accurate records is essential in defending legal or medical queries that may arise, ensuring that facilities meet both ethical and legal standards for resident care.
Examples of Using the Report of Resident Physical Examination
Several scenarios illustrate the practical use of the Report of Resident Physical Examination:
- New Admissions: Before admission, residents undergo a physical examination to tailor their living arrangements according to their health requirements.
- Change in Health Status: If a resident experiences a significant change in health, the report is revisited to adjust care plans accordingly.
- Regulatory Assessments: Regular checks by health inspectors require access to these reports to ensure compliance with assisted living standards.
Overall, the report is a vital tool in managing and delivering resident care effectively within assisted living environments.
