


Definition and Meaning of Authorization for the Use and Disclosure of Health - Dphhs
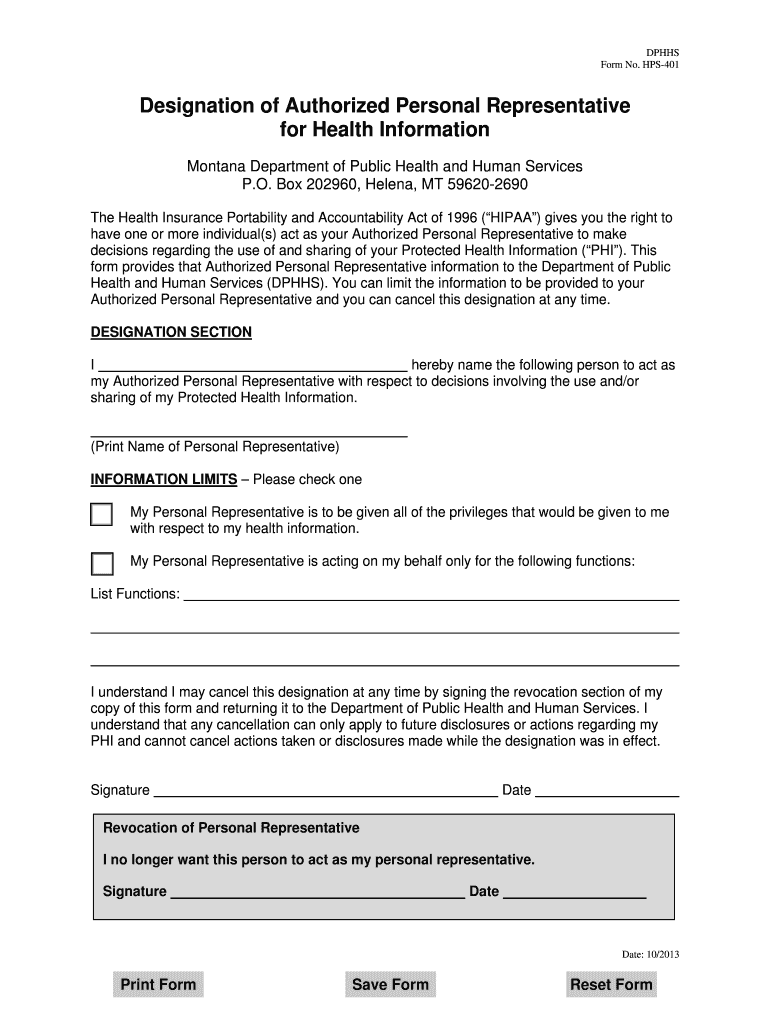
The "Authorization for the Use and Disclosure of Health - Dphhs" form is a legal document issued by the Montana Department of Public Health and Human Services (DPHHS). This form allows individuals to authorize the sharing and use of their Protected Health Information (PHI) in compliance with the Health Insurance Portability and Accountability Act (HIPAA). The form designates an Authorized Personal Representative who can make health-related decisions on behalf of the individual. It ensures that sensitive health information is disclosed only to authorized personnel, safeguarding the individual's privacy and providing clarity on who can access specific health details.
Key Elements of the Authorization Form
Several crucial elements make up the "Authorization for the Use and Disclosure of Health - Dphhs" form, ensuring it serves its intended purpose:
- Authorized Personal Representative: The designated individual who is granted access to the individual's PHI and can make decisions regarding its use and disclosure.
- Scope of Authorization: Clear definitions of what health information can be shared, and with whom, are imperative for maintaining privacy. This may include medical records, treatment plans, or billing information.
- Revocation Rights: Individuals retain the right to revoke or modify their authorization at any time, with the understanding that revocation does not apply retroactively.
- Expiration Date: The authorization is valid until a specified date, after which the rights granted through the form are no longer applicable.
How to Use the Authorization Form
To effectively use the form, individuals should:
- Identify Information to Share: Determine which parts of their PHI they wish to disclose.
- Select an Authorized Representative: Choose someone they trust to handle their health information.
- Define the Purpose: Specify the reasons and circumstances under which the information can be utilized or disclosed.
- Sign and Date the Form: Ensure the form is completed with all required signatures to be legally valid.
The document must be completed accurately to ensure legal compliance and protection of sensitive health data.
Steps to Complete the Authorization Form
- Personal Information: Enter personal details such as name, address, and date of birth to ensure the document is traceable to the correct individual.
- Specify Health Information: Clearly outline what information can be disclosed and for what purpose.
- Authorized Individual Information: Provide details of the person designated to access the health information.
- Set Expiration Date and Conditions: Choose an expiration date for the authorization and any conditions under which it becomes void.
- Signatures: Obtain necessary signatures from both the individual and the authorized representative.
Importance of Authorizing Health Information Disclosure
Using the authorization form is crucial for:
- Privacy Protection: Ensures that PHI is only shared with and used by trusted individuals.
- Medical Decision Support: Allows designated representatives to access necessary information to make informed health decisions on an individual’s behalf.
- Compliance with HIPAA: Helps maintain compliance with legal and regulatory requirements for health information sharing.
Who Typically Uses the Authorization Form?
The form is commonly utilized by:
- Patients: To grant access to their health data for specific purposes.
- Healthcare Providers: To obtain necessary consent for sharing patient information.
- Legal Representatives: When managing the health-related affairs of individuals unable to make their own decisions due to age or incapacity.
These users rely on the form to facilitate the lawful sharing of healthcare information.

Legal Use and Compliance of the Authorization Form
The legal compliance aspect of this form ensures it aligns with HIPAA regulations, protecting patient confidentiality while allowing necessary access to information. Legal representatives use this form to legally permit the use and disclosure of sensitive information without breaching privacy laws.
Examples of Using the Authorization Form
Real-world scenarios include:
- Patient Transfers: Facilitating the transfer of medical records to new healthcare providers as patients move or change providers.
- Legal Proceedings: Enabling legal representatives to access pertinent health information for court cases.
- Family Health Management: Allowing family members to manage the healthcare needs of incapacitated or chronically ill relatives.
The form ensures these processes are executed transparently and legally.