


Definition & Meaning
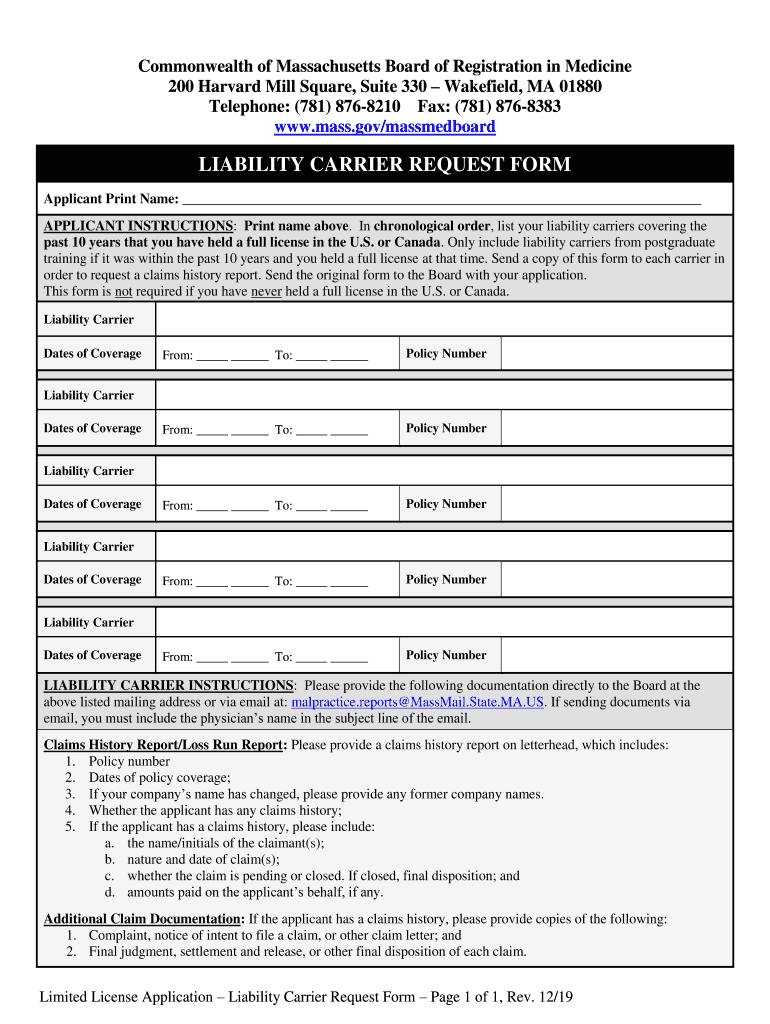
The "Liability Carrier Request Form" is a document utilized by the Commonwealth of Massachusetts Board of Registration in Medicine to verify an applicant's insurance history. It requires applicants to detail their liability coverage over the past ten years. This form is instrumental in providing the board with necessary claims history reports, ensuring that applicants have maintained appropriate professional liability coverage throughout their career. Understanding its significance ensures compliance with medical board requirements and mitigates the risk of application denial due to missing liability information.
How to Use the Liability Carrier Request Form
The proper use of the Liability Carrier Request Form involves a sequential process. First, applicants must list all liability carriers that provided coverage within the specified time frame. Clear guidelines are provided for submissions to each carrier, emphasizing the need for detailed claims history reports. Applicants must then consolidate these reports and submit them to the medical board along with their application. This structured approach ensures that all necessary information is relayed accurately, facilitating a smoother application review process.
How to Obtain the Liability Carrier Request Form
The form is readily accessible through the Massachusetts Board of Registration in Medicine's website. Detailed instructions for download and completion are included to assist applicants in acquiring the document. Alternatively, candidates may request the form via mail or email, if electronic access proves challenging. Ensuring that the correct version of the form is obtained is crucial, as updates may occur to reflect changes in regulatory requirements or submission procedures.
Steps to Complete the Liability Carrier Request Form
-
Gather Personal Information: Begin by collecting personal details, including full name, contact information, and professional identification numbers.
-
List Liability Carriers: Provide a comprehensive list of all liability insurers from the past ten years, including policy numbers and coverage periods.
-
Request Claims History Reports: Contact each liability carrier to request detailed claims history reports, following the board's guidelines for information inclusion.
-
Compile Documents: Once received, compile all claims reports into a cohesive application packet.
-
Submit to the Board: Send the completed form and supporting documents to the Board of Registration in Medicine via their specified submission methods.
Key Elements of the Liability Carrier Request Form
The form comprises several critical sections:
- Identification Details: Applicant's professional and personal identifiers.
- Insurance History: Names, contact information, and policy details of each liability carrier.
- Claims Information: Specifics of claims, if any, including dates, outcomes, and associated policy details.
- Supplementary Instructions: Guidelines for both applicants and carriers on information requirements for claims history reports.
Legal Use of the Liability Carrier Request Form
The form is a legally binding document required by the Massachusetts Board of Registration in Medicine as a part of the medical licensure application process. It ensures that healthcare professionals have met necessary liability coverage standards. Misrepresentation or omission of liability history on this form can result in significant legal consequences, including denial of licensure or revocation of existing licenses. Compliance with all aspects of the form's requirements is paramount to maintaining professional standing.
Important Terms Related to the Liability Carrier Request Form
- Claims History Reports: Comprehensive accounts provided by insurers detailing any claims made against the insured individual.
- Liability Coverage: Insurance coverage that protects against claims alleging that one's negligence or inappropriate action resulted in bodily injury or property damage.
- Policy Number: A unique identifier for an insurance contract between the insurer and the insured.
Who Typically Uses the Liability Carrier Request Form
The primary users of this form are medical practitioners applying for initial licensure or renewal in Massachusetts. It is also relevant for medical staff or administrators responsible for managing the licensure process within healthcare institutions. Ensuring accurate completion and submission of this form is critical for professionals to practice legally within the state, safeguarding both their careers and the institutions they represent.