Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send 844 559 3471 via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out 18005456962 with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
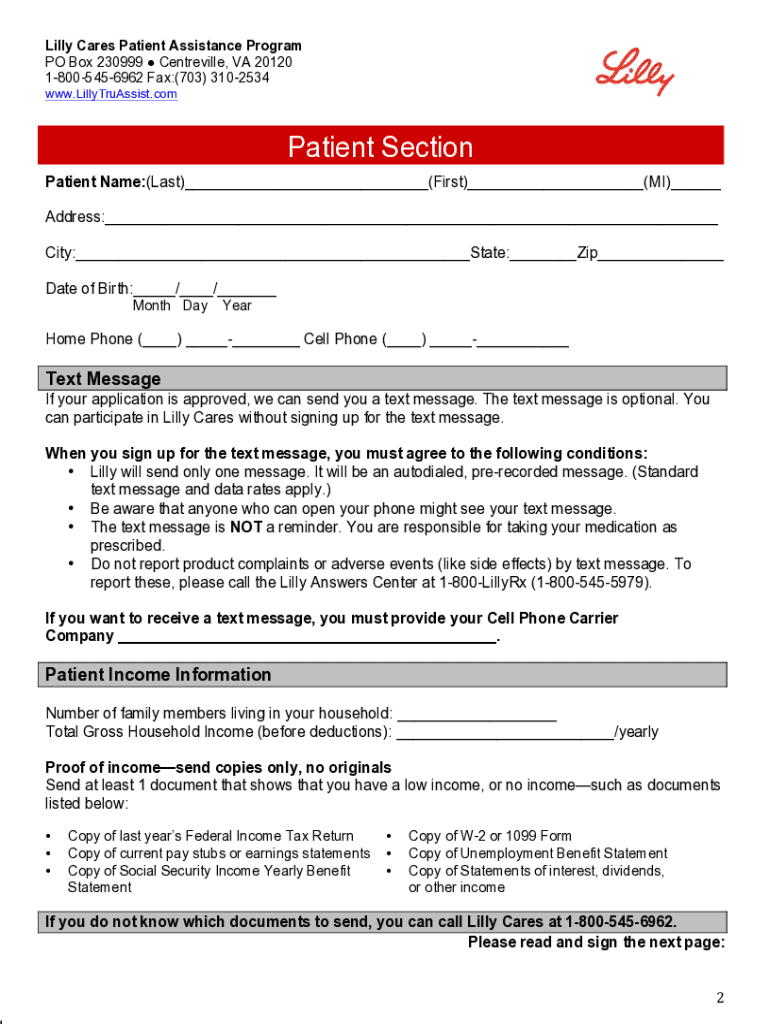
Click ‘Get Form’ to open the Lilly Cares Patient Assistance Program application in the editor.
Begin by filling out the Patient Section. Enter your name, address, date of birth, and contact information accurately.
In the Patient Income Information section, indicate the number of family members and your total gross household income. Ensure you have proof of income documents ready to upload.
Review the Patient Certification carefully. Confirm that all statements are true and sign where indicated.
Next, have your doctor complete the Doctor Section. They will need to provide their details and confirm your eligibility for the program.
Once both sections are completed, save your form and either mail or fax it along with copies of your proof-of-income documents to the Lilly Cares program using the provided contact information.
Start filling out your application today for free on our platform!
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.