Related links
AFLAC: Hospital Indemnity Claim Form
HOSPITAL INDEMNITY CLAIM FORM. Thank you for trusting Aflac with your Hospital Indemnity needs. ➢ If you are interested in filing your claim online orRead more
Learn more
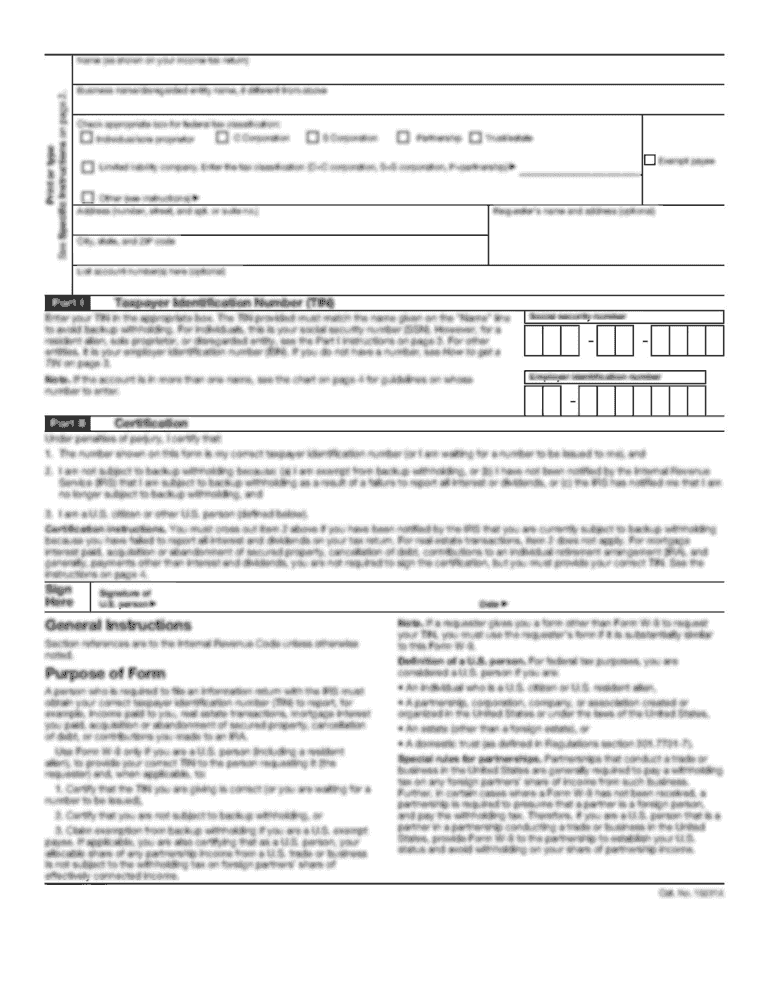
Revised 1500 Claim Form Instructions
by JB Doe The National Uniform Claim Committee (NUCC) released a revised 1500 Claim Form, which is commonly referred to as the CMS-1500. The revised CMS-1500 (02/12)Read more
Learn more
HOSPITAL INDEMNITY CLAIM FORM
Please sign the attached HIPAA Form and return it with the completed claim form. If filing a claim within the first policy year for benefits, medical recordsRead more
Learn more