We've got more versions of the family medical leave act form form. Select the right family medical leave act form version from the list and start editing it straight away!
FMLA form (PDF)Intermittent FMLA form pdfPrintable FMLA formsPrintable FMLA forms for Family memberVA FMLA form pdfFMLA forms for EmployeeFMLA medical certification formWhat conditions qualify for FMLA leave
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
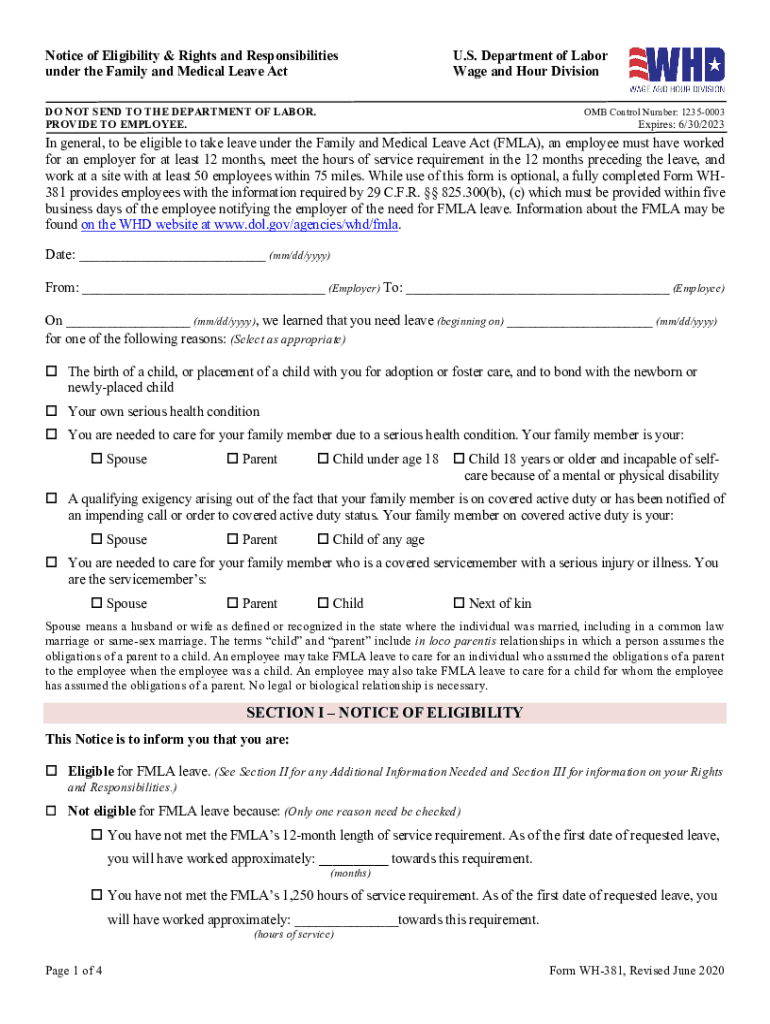
Family and Medical Leave Act (FMLA) Procedures and Forms
To request FMLA Leave submit the Request for Family and Medical Leave Act (FMLA) Form to the Office of Human Resources for processing at least 30 days beforeRead more
Family members serious health condition, form WH-380-F - Use when a leave request is due to the medical condition of the employees family member. Condicin deRead more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.