emory medical records release
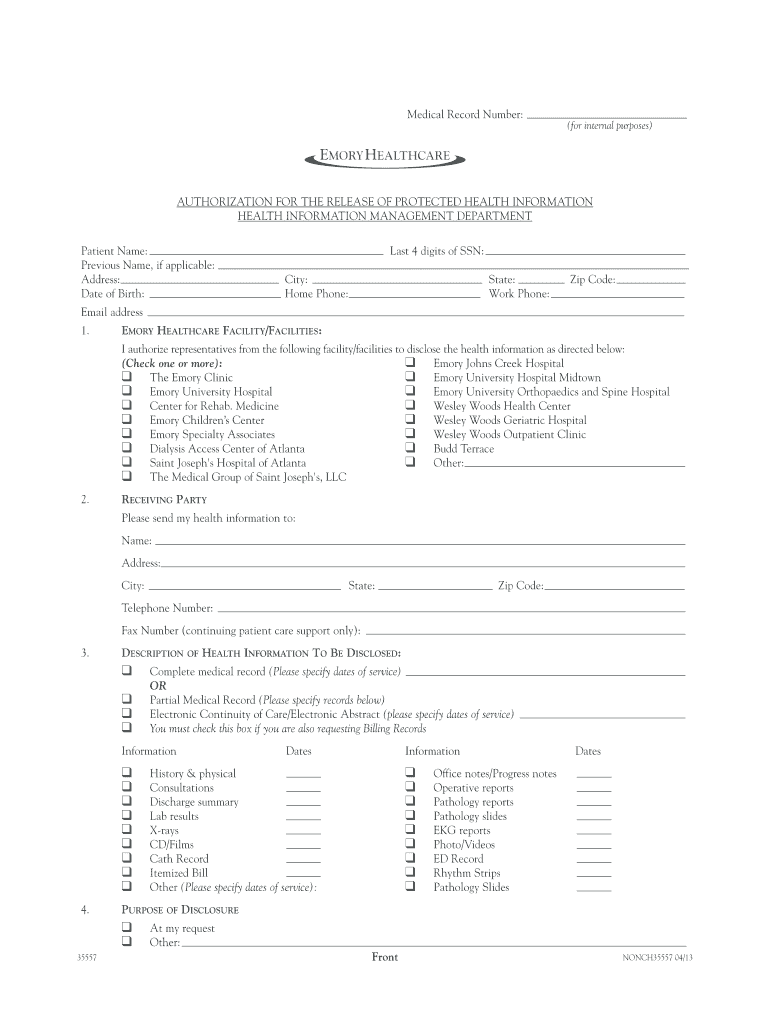
authorization for the release of protected health information
I hereby release Emory. University and its affiliated entities, including but not limited to Emory Healthcare, Inc., Emory University Hospital, Emory.Read more
Learn more
Emory University Consent to be a Research Subject and
Sep 27, 2018 Copies of the consent form/HIPAA authorization that you sign will be put in your Emory Healthcare medical record. Emory Healthcare may createRead more
Learn more
Lambert-GA | Integrated Human Practices
Participants in all surveys provided signed consent for the release of their responses from themselves or a legal guardian. Additionally, participants inRead more
Learn more