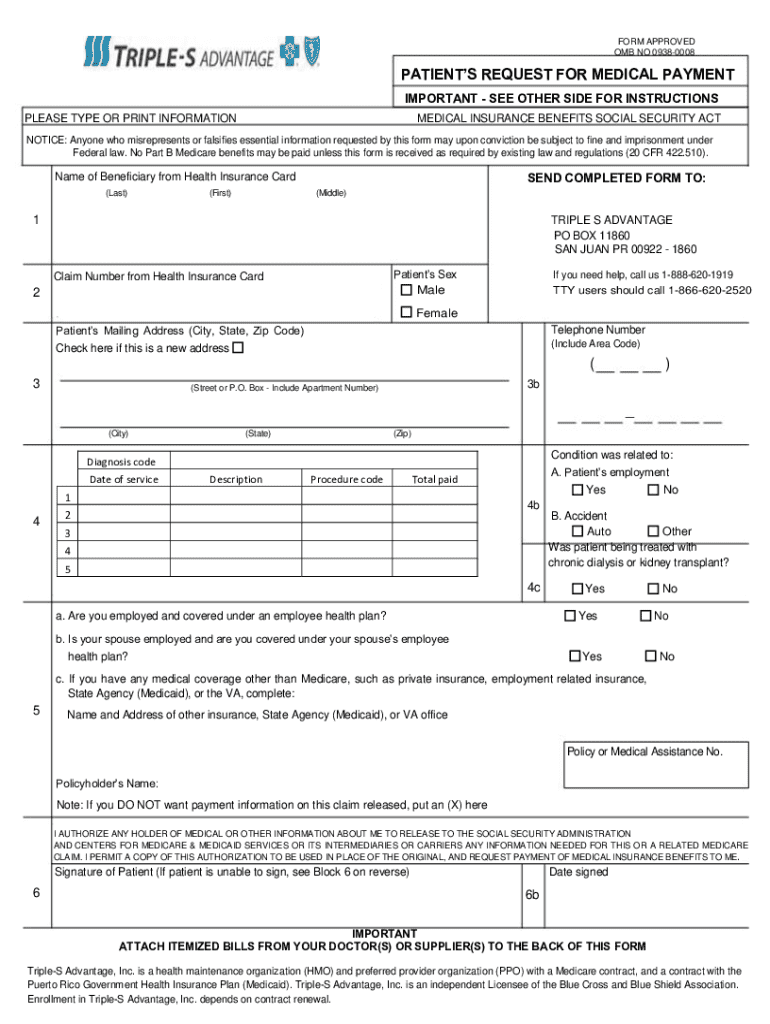



Definition and Purpose of the Patient's Request for Medical Payment
The Patient's Request for Medical Payment form is an essential Medicare document that allows patients to request reimbursement for medical expenses incurred. It facilitates the process for individuals to claim payment for services they have paid for out-of-pocket, ensuring that the Medicare system accurately acknowledges these expenses. This form is particularly relevant for those who experience difficulties with medical billing or discrepancies in service charges.
How to Use the Patient's Request for Medical Payment
To effectively use the Patient's Request for Medical Payment, follow these structured steps:
-
Collect Necessary Information: Before filling out the form, gather all relevant personal and insurance details, invoices, and proof of payment documentation. This ensures you have everything you need to complete the form accurately.
-
Accurate Form Completion: Carefully enter both personal details and information about the medical services provided. This includes date of service, provider details, and the amount paid.
-
Attach Required Documentation: Attach copies of all necessary documents, such as invoices and receipts, to substantiate the claim.
-
Submit the Completed Form: The form and accompanying documents should be submitted according to the specific instructions provided, usually by mail to Triple-S Advantage in Puerto Rico or as otherwise directed by your Medicare provider.
-
Follow-up: After submission, it's crucial to track the status of your request to ensure it is processed and to address any additional inquiries from Medicare.
Steps to Complete the Patient's Request for Medical Payment
Completing the form involves several precise steps:
-
Personal Information Section: Enter your full name, Medicare number, and contact information as requested.
-
Medical Service Details: Specify the nature of the medical service received, including the date and the provider's name and address.
-
Expense Details: Provide an itemized list of services with respective costs. This section must match the invoiced amounts to avoid discrepancies.
-
Signature and Date: Sign and date the form, confirming the authenticity of the information provided.
-
Review and Submission: Double-check all filled sections for completeness and accuracy before submitting.
Key Elements of the Patient's Request for Medical Payment
The form incorporates several crucial components:
- Personal and Insurance Information: Identifies the patient and connects the form to their specific Medicare account.
- Details of Medical Services: Describes the services for which reimbursement is being requested.
- Provider Information: Includes the healthcare provider's name and address to verify service legitimacy.
- Costs Incurred: Lists specific financial amounts along with supporting documentation to validate the request.
- Patient’s Certification: Provides an area for the patient to attest to the truthfulness of their claim.
Required Documents for Submission
To complete the process, the following documents are typically required:
- Invoices from Healthcare Providers: Detailed invoices showing the services rendered.
- Proof of Payment: Receipts or payment confirmations to demonstrate that the patient has made out-of-pocket payments.
- Insurance Explanation of Benefits (EOB): If available, this should detail what has already been covered by insurance.
Who Typically Uses the Patient's Request for Medical Payment
This form is primarily used by Medicare beneficiaries who need to claim reimbursements for out-of-pocket expenses when:
- Medicare does not directly pay the provider for services rendered.
- There are discrepancies in billing directly related to Medicare-covered services.
- Immediate payment was required at the point of service, and Medicare reimbursement is sought afterward.

Legal Use and Compliance with the Patient's Request for Medical Payment
When using this form, legal compliance is paramount:
- Accuracy is Crucial: It is necessary to provide accurate and truthful information, as discrepancies can lead to legal consequences.
- Following Medicare Guidelines: Ensure that all Medicare guidelines are adhered to, including the types of services eligible for reimbursement.
Important Terms Related to the Patient's Request for Medical Payment
Understanding these terms can assist in completing the form accurately:
- Medicare Number: The unique identification number assigned to each Medicare beneficiary.
- Explanation of Benefits (EOB): A statement provided by Medicare, detailing what costs it covers.
- Out-of-Pocket Expenses: Costs that have been paid directly by the patient for medical services.
These sections ensure comprehensive coverage of the form's purpose, usage, and related processes, enhancing understanding and application in real-world scenarios.