Does everyone have to pay $170 a month for Medicare?
Do you have to pay for Medicare? Yes, most people pay $185 per month for Medicare Part B and may pay more if they choose extra coverage options. Part A is free if you worked for 10 years or more.
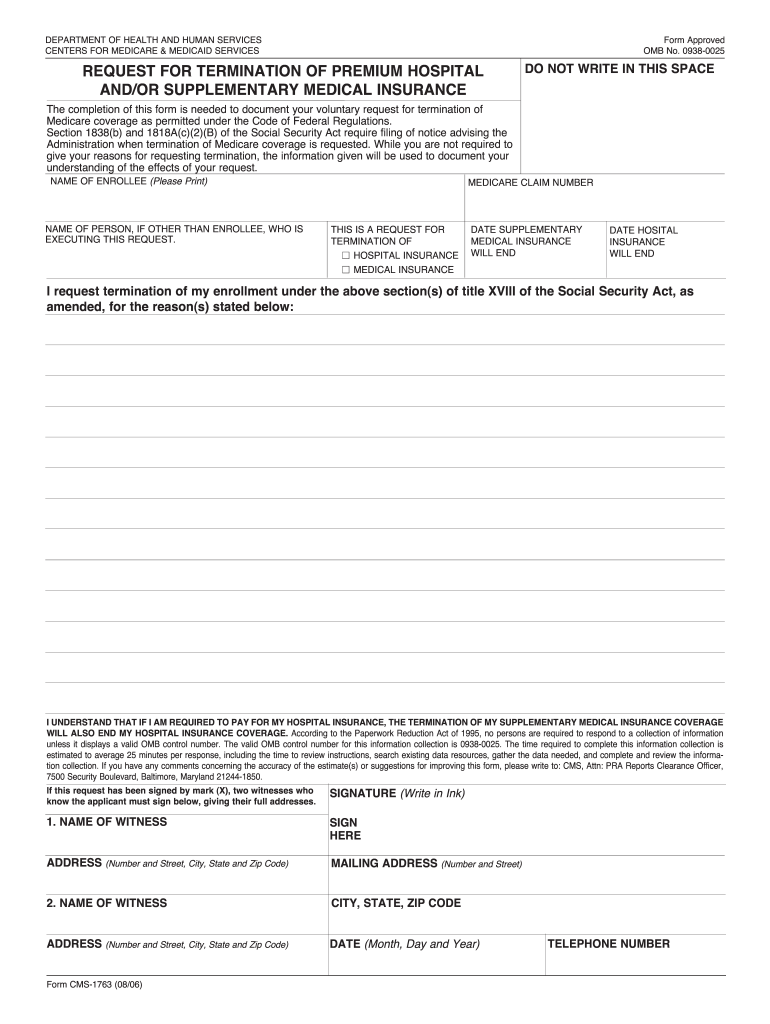
What is form CMS 1763 used for?
Use this form: If you have premium Part A or Part B, but wish to no longer be enrolled. If you have Part B, but recently re-joined the workforce with access to employer-sponsored health insurance and wish to voluntarily terminate this coverage.
What is the CMS 1763 form?
CMS 1763. Form Title. Request for Termination of Premium Hospital Insurance of Supplementary Medical Insurance.
Can I submit form CMS 1763 online?
How to fill out Form CMS 1763? Name of Enrollee. Medicare Number. Name of the Person, if Other than Enrollee, Who Is Executing the Request (if appropriate). This is a Request for Termination of Hospital Insurance/Medical Insurance. Date Hospital Insurance Will End. Reasons for the termination request.
how to cancel medicare part b
CMS-40BCms 1763 formCms 1763 instructionsCMS-1763 form downloadCMS-1763 form PDFCMS-1763 Form 2025Where to send form CMS-1763Where do i fax my Social Security form CMS-1763
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
May 15, 2009 CMS-1763 is a standardized form for Medicare enrollees to request termination of Part B and/or premium Part A coverage, to ensure understanding
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.