Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send form cms 1763 via email, link, or fax. You can also download it, export it or print it out.
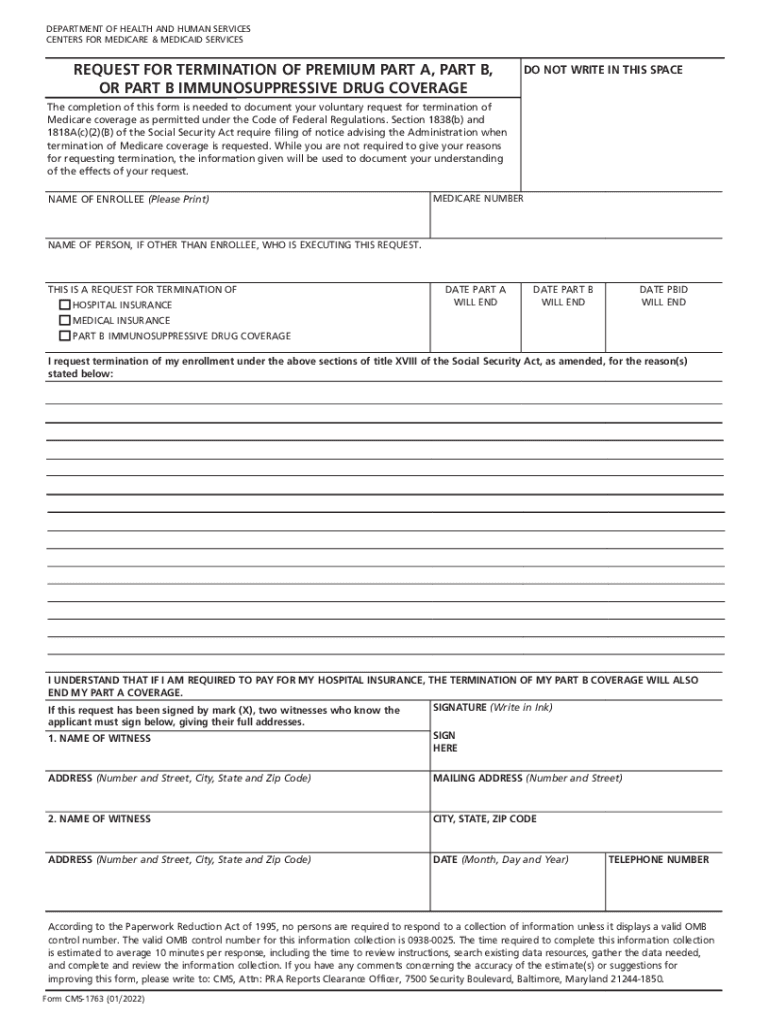
How to use or fill out FORM CMS 1763, REQUEST FOR TERMINATION OF PREMIUM PART A, PART B, OR PART B IMMUNOSUPPRESSIVE DRUG C with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
Click ‘Get Form’ to open it in the editor.
Begin by entering your name and Medicare number in the designated fields. Ensure that all information is accurate to avoid processing delays.
Indicate whether you are requesting termination for Hospital Insurance, Medical Insurance, or Part B Immunosuppressive Drug Coverage by checking the appropriate boxes.
Fill in the dates for when you wish each coverage to end. This is crucial for ensuring your request is processed correctly.
If applicable, provide a witness signature if you signed with an 'X'. Two witnesses must sign and provide their addresses.
Review all entered information for accuracy before submitting. Use our platform’s tools to make any necessary edits easily.
Once completed, download the form and send it to your local Social Security office as instructed.
Start using our platform today to fill out FORM CMS 1763 quickly and efficiently!
Fill out FORM CMS 1763, REQUEST FOR TERMINATION OF PREMIUM PART A, PART B, OR PART B IMMUNOSUPPRESSIVE DRUG C online It's free
See more FORM CMS 1763, REQUEST FOR TERMINATION OF PREMIUM PART A, PART B, OR PART B IMMUNOSUPPRESSIVE DRUG C versions
We've got more versions of the FORM CMS 1763, REQUEST FOR TERMINATION OF PREMIUM PART A, PART B, OR PART B IMMUNOSUPPRESSIVE DRUG C form. Select the right FORM CMS 1763, REQUEST FOR TERMINATION OF PREMIUM PART A, PART B, OR PART B IMMUNOSUPPRESSIVE DRUG C version from the list and start editing it straight away!
The standard monthly premium for Medicare Part B enrollees will be $185.00 for 2025, an increase of $10.30 from $174.70 in 2024. The annual deductible for all Medicare Part B beneficiaries will be $257 in 2025, an increase of $17 from the annual deductible of $240 in 2024.
What is the form for Medicare Part B disenrollment?
How do you cancel Medicare Part B? Youll simply need to mail or fax a signed Form CMS-1763 (a request for termination of premium hospital insurance or supplementary medical insurance) to Social Security.
What is a Form 40 B for Medicare?
This form is your application for Medicare Part B (Medical Insurance).
What is the CMS 1763 form to cancel Medicare Part B?
Fill out Request for Termination of Premium Hospital Insurance of Supplementary Medical Insurance (Form CMS-1763) (PDF) and fax or mail it to your local Social Security office. You can cancel Part A only if you pay a premium for it. You can cancel Part B at any time.
How to opt out of Medicare Part B as a provider?
To opt-out, you must: Submit an opt-out affidavit to Medicare. Enter into a private contract with each of your Medicare patients. This contract will reflect the agreement between you and your Medicare patients that they will pay for services out of pocket, and that nobody will submit the bill to Medicare for payment.
social security form cms 1763
cms-1763 form to cancel medicare part bWhere do I fax my Social Security form CMS 1763Sample letter to cancel Medicare Part BSample letter to cancel Medicare Part B pdfWhere to send form CMS-1763how to fill out form cms-1763Printable Form CMS 1763How to submit form CMS 1763
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
This form is used for proof of group health care coverage based on current employment. This information is needed to process your Medicare enrollment application.
Is there a form for Medicare Part B?
You can apply online or you can mail your completed CMS 40B, Application for Enrollment in Medicare - Part B (Medical Insurance) to your local Social Security office.
cms 1763 form
86-9811-20PD 200007 Solutions Evidence of Coverage:
Our plan only covers Medicare Parts A, B, and D services and drugs that are request is for a Medicare Part B prescription drug. If you believe we
This form, titled Request for Termination of Premium Part A, Part B, or Part D. Immunosuppressive Drug Coverage, is required to formally process your request.
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.