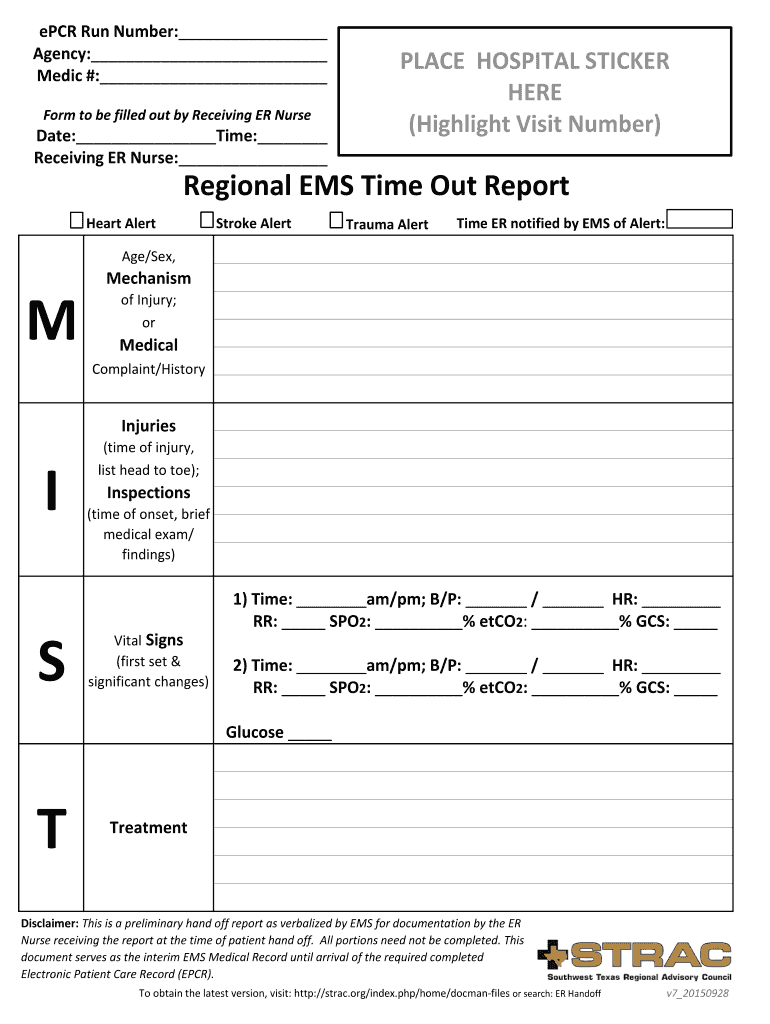
Definition and Meaning of the ER Nurse Report Sheet
The ER nurse report sheet is a critical tool used in emergency rooms for documenting patient information during handoffs between nursing staff. It is designed to ensure a smooth transition of care, maintain continuity, and provide important data needed for effective patient management. The sheet typically includes essential fields such as patient identification, presenting complaints, vital signs, and treatment information. This document serves as a reference point for healthcare providers to make informed clinical decisions rapidly.
The importance of this report sheet cannot be overstated, as it facilitates communication among team members and ensures that vital details are not overlooked during handoff. The structured format helps in reducing the likelihood of errors, which can be crucial in emergent situations. By setting a standard for what information is shared, it also helps to streamline workflow in a busy emergency department.
Key Elements of the ER Nurse Report Sheet
An effective ER nurse report sheet should contain several key elements that facilitate comprehensive patient assessment and treatment planning. Below are some of the fundamental sections to include:
-
Patient Identification Information
- Full name, age, sex, and medical record number.
- Contact information and emergency contacts.
-
Chief Complaint and History of Present Illness
- A concise statement of the issue that brought the patient to the ER.
- Relevant medical history that may impact treatment options.
-
Vital Signs and Assessment Data
- Documented initial vital signs, including blood pressure, heart rate, respiratory rate, and temperature.
- Any relevant lab results or imaging findings, when available.
-
Triage Information
- Initial patient assessment categorization based on the urgency of care needed.
- Any additional pertinent details that may affect triage decisions.
-
Treatment Provided and Response
- Details regarding any interventions performed prior to or upon arrival at the ER.
- Patient response to the treatment, including any changes in condition.
-
Plan of Care and Follow-Up Needs
- Recommendations for further treatment or diagnostic measures.
- Discharge instructions or referrals, if applicable.
Including these elements ensures that both the receiving and treating nurses have a clear and comprehensive understanding of the patient's situation, leading to informed, timely care.
Steps to Complete the ER Nurse Report Sheet
Completing an ER nurse report sheet involves systematic steps to ensure accuracy and thoroughness. Here are the essential steps:
-
Gather Patient Information
Collect basic details such as patient name, age, and medical history. Ensure that this information is current and matches that in the hospital database. -
Document Vital Signs
Measure and record vital signs accurately. Use an appropriate format to ensure consistency, and note any significant changes from prior measurements. -
Record the Chief Complaint
Clearly write down the patient's chief complaint as expressed. This should reflect the primary reason for the emergency visit. -
Log Any Treatments Administered
Detail any treatments provided prior to or during the patient's ED visit. This might include medications administered, procedures done, or diagnostic tests ordered. -
Assess and Document Findings
Reflect on the nurse's observations and assessments, including the patient's response to treatment. Use specific terminology to describe findings accurately. -
Outline the Follow-Up Plan
Include recommendations for further tests, treatments, or follow-up consultations. Ensure that any discharge instructions are clearly written out for the patient's understanding.
Following these steps will help health care providers complete the report sheet efficiently and completely, ensuring that all critical information regarding patient care is conveyed.
Legal Use of the ER Nurse Report Sheet
The ER nurse report sheet holds significant legal importance in healthcare settings. It serves as an official record of patient care and can play a key role in legal proceedings or audits. To ensure its legal use, consider the following aspects:
-
Accuracy is Critical
Each entry on the report sheet must reflect the true and accurate information. Misrepresentation or omission of data could lead to liability issues. -
Signatures and Authentications
Proper documentation often requires signatures of staff members who completed or reviewed the report. This creates a chain of accountability. -
Retention Policies
Compliance with hospital and legal standards for retaining medical documentation is crucial. These policies detail how long such records must be kept and in what format. -
Confidentiality Compliance
Patient confidentiality laws, such as HIPAA, dictate how patient information should be handled. All staff must be trained to recognize and uphold these legal standards.
Adhering to these legal guidelines strengthens the integrity of the ER nursing process and supports a reliable healthcare delivery system.
Examples of Using the ER Nurse Report Sheet
Utilizing an ER nurse report sheet can significantly enhance clinical efficiency and patient safety. Here are practical scenarios demonstrating its application:
-
Trauma Patient Handoff
When a trauma patient arrives, the report sheet allows quick entry of vital information. For example, upon receiving a motorcycle accident victim, the nurse quickly documents the patient's loss of consciousness, vital signs indicating hypotension, and details of initial interventions—like fluid resuscitation or imaging orders. -
Multi-Patient Triage Situation
In cases where multiple patients arrive simultaneously, such as during a surge in respiratory illness, nurses use the report sheets to rapidly organize and prioritize care based on presenting conditions and vital sign abnormalities. This standardized approach facilitates immediate and effective intervention. -
Interdisciplinary Communication
When handing off care from the ED to a hospital ward, the report sheet serves to transfer critical information succinctly. For instance, if a patient requires a bed assignment due to a severe infection, the documented nursing assessment, treatment history, and cognitive status provide the receiving nurse with essential insight for continued care.
These examples highlight how the ER nurse report sheet is not just a documentation tool but an integral component of the communication framework within healthcare facilities.