Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send it via email, link, or fax. You can also download it, export it or print it out.
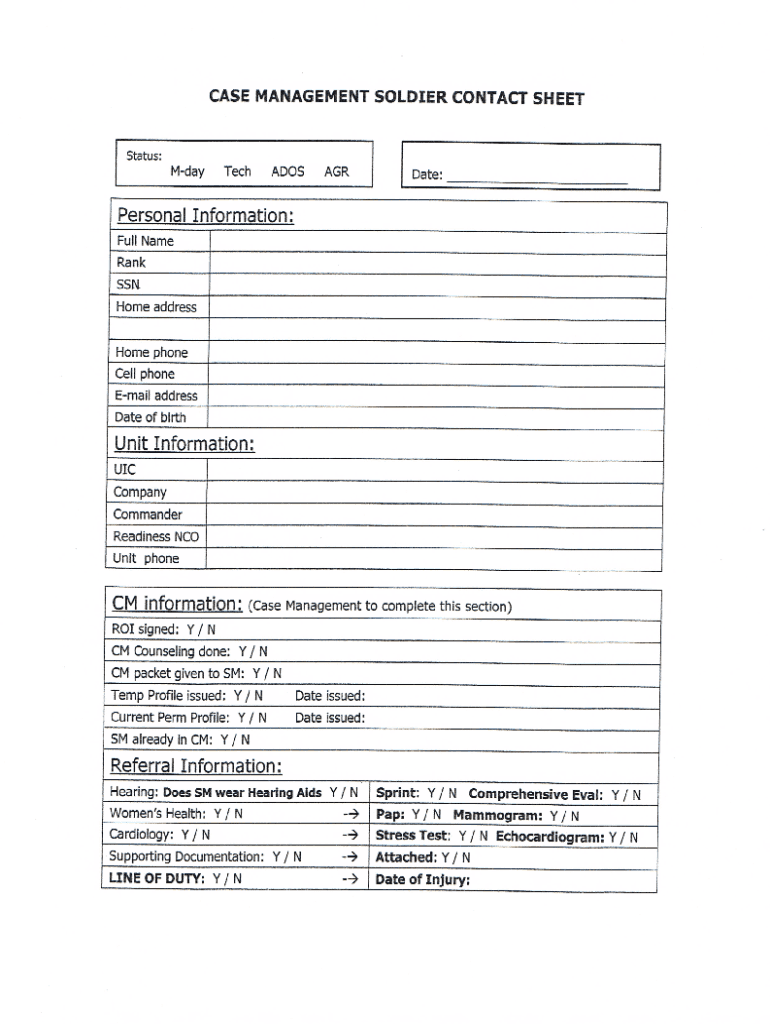
How to use or fill out dd form 2870 with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
Click ‘Get Form’ to open the dd form 2870 in the editor.
Begin by entering your personal information in Section I. This includes your name, address, and contact details. Ensure all information is accurate for processing.
Move to Section II, where you will specify the type of request you are making. Select the appropriate option that aligns with your needs.
In Section III, provide any additional information required for your request. This may include details about the service or records you are seeking.
Finally, review all sections for completeness and accuracy. Use our platform’s editing tools to make any necessary adjustments before signing.
Start using our platform today to fill out your dd form 2870 easily and for free!
Dd form 2870 pdfDD form 2870 PDF download freePrintable DD Form 2870 downloadDD FORM 2870 army pubsDD Form 2870 TRICAREDD FORM 2870 2024DD form 2870 NOV 2023DD Form 2870 instructions
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
DD FORM 2870, DEC 2003. AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION. PRIVACY ACT STATEMENT. In accordance with the Privacy Act of 1974Read more
DD Form 2870, Authorization for Disclosure of Medical or
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/Read more
Complete reductive dechlorination of 1,2-dichloropropane
The transformation of 1,2-dichloropropane (1,2-D) was observed in anaerobic microcosms and enrichment cultures derived from Red Cedar Creek sediment.Read more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.