Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send it via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out 1997 ca 17 form with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
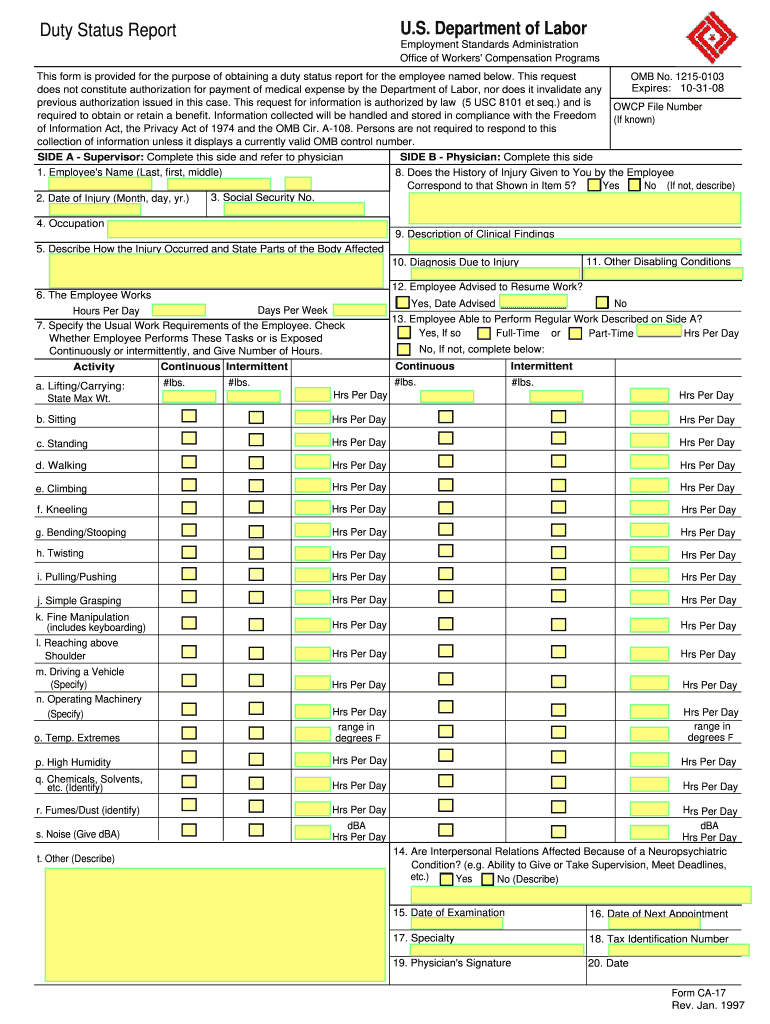
Click ‘Get Form’ to open the 1997 ca 17 form in the editor.
Begin by filling out Side A, which requires the supervisor's details. Enter the employee's name, social security number, and date of injury.
In Section 4, specify the employee's occupation and provide a detailed description of how the injury occurred in Section 5.
Complete Section 6 by indicating the employee's work schedule, including days per week and hours per day.
For Sections 7 through 14, check off whether the employee performs specific tasks and indicate hours spent on each activity. Be thorough in documenting any disabling conditions.
Once all sections are completed, ensure that Side B is filled out by a physician. This includes clinical findings and diagnosis due to injury.
Finally, review all entries for accuracy before saving or sending the completed form directly from our platform.
Start using our platform today to fill out your forms online for free!
1997 ca 17 form pdfPrintable CA-17 form PDFHow to fill out a 1997 ca 17 formCA-17 form post officeCurrent CA 17 form1997 ca 17 form download1997 ca 17 form onlineCA 17 fillable form
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
Quality of Source Water from Public-Supply Wells in the
Appendix 17. Comparison Among Percentages of Public Wells or Public Water Systems with Concentrations Greater Than Human-Health Benchmarks for Regulated.Read more
U. S. Department of Labor Notice of Occupational Disease
Cited by 13 I DocHub, under penalty of law, that the disease or illness described above was the result of my employment with the United States.Read more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.