Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send it via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out BlueCare Plus (HMO SNP)SM Home Health Request Fax Form with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
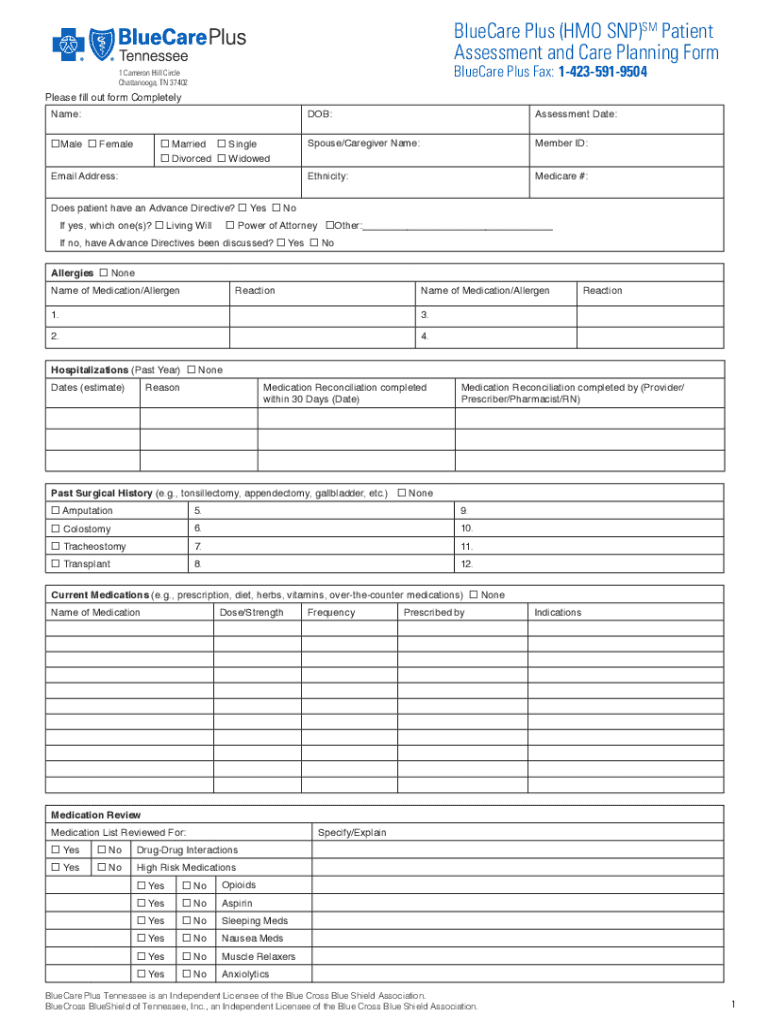
Click ‘Get Form’ to open the BlueCare Plus (HMO SNP)SM Home Health Request Fax Form in the editor.
Begin by entering the patient's name, gender, marital status, and email address in the designated fields. Ensure accuracy as this information is crucial for identification.
Fill in the date of birth and assessment date. Next, provide details about the spouse or caregiver's name and member ID.
Indicate whether the patient has an Advance Directive by selecting 'Yes' or 'No'. If applicable, specify which type(s) of directive exist.
Document any allergies and reactions by listing medications or allergens in the provided sections. This helps healthcare providers understand potential risks.
Complete sections on hospitalizations, current medications, and past surgical history. Be thorough to ensure comprehensive care planning.
Review all entries for accuracy before saving your work. Utilize our platform’s features to easily edit any mistakes.
Start using our platform today to streamline your form completion process for free!
Fill out BlueCare Plus (HMO SNP)SM Home Health Request Fax Form online It's free
See more BlueCare Plus (HMO SNP)SM Home Health Request Fax Form versions
We've got more versions of the BlueCare Plus (HMO SNP)SM Home Health Request Fax Form form. Select the right BlueCare Plus (HMO SNP)SM Home Health Request Fax Form version from the list and start editing it straight away!
Title Page The software version is 2019.2. The release date is
Deny Medicaid/Family Health Plus/FHP-PAP/FPBP,Client Request (WRITTEN). We have denied your application for Medicaid/FHP/FHP-PAP/FPBP. This is.Read more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.