Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send form pa 635 via email, link, or fax. You can also download it, export it or print it out.
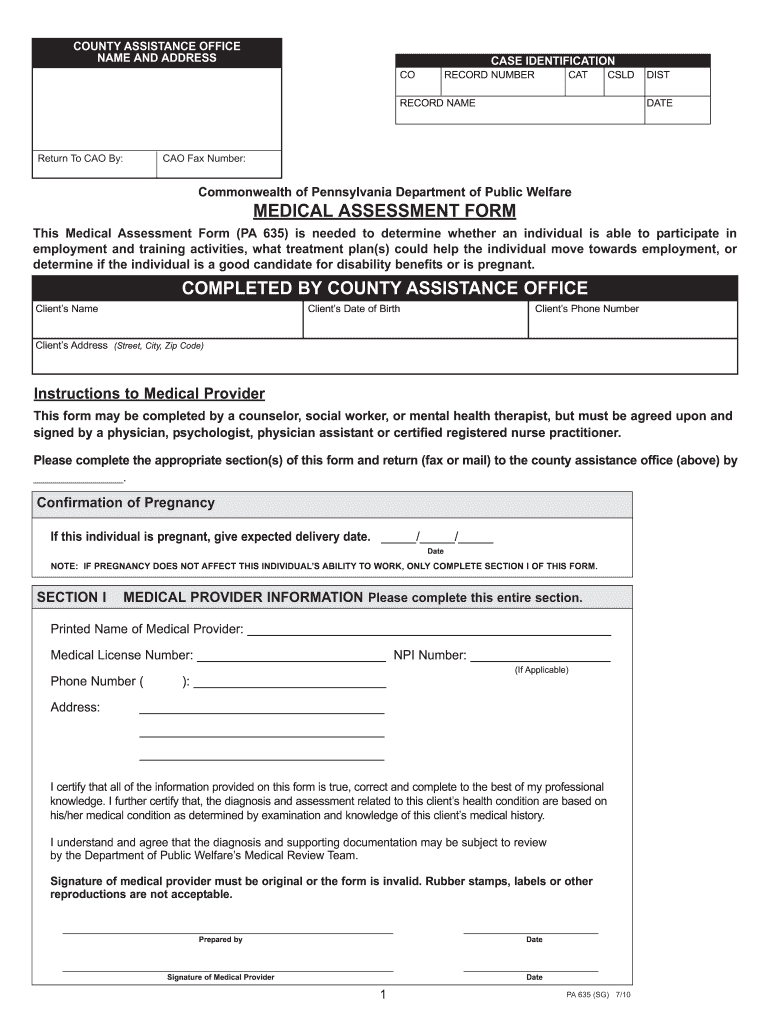
How to use or fill out PA Medical Form with DocHub
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
Click ‘Get Form’ to open the PA Medical Form in our editor.
Begin by entering the client’s name, date of birth, phone number, and address in the designated fields. Ensure accuracy as this information is crucial for identification.
In Section I, the medical provider must fill out their information including printed name, medical license number, and contact details. This section requires a signature from a qualified medical professional.
Proceed to Section II where you will assess employability. Select the appropriate checkbox based on the individual's capabilities and provide any necessary accommodations or treatment plans.
In Section III, document all relevant diagnoses along with their ICD-9 codes. Clearly explain how each diagnosis impacts the client's ability to work.
Review all entries for completeness and accuracy before saving your changes. Once finalized, you can easily share or print the form directly from our platform.
Start using our platform today to fill out your PA Medical Form quickly and efficiently!
Pa medical form pdfPa medical form templatePrintable Medical Assessment Form (PA)Pa 1663 form pdfPennDOT medical form for permitForm (PA 635 or 1663)Pa medical form onlinePenndot Medical reporting form
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
Medical Reporting Forms | Driver and Vehicle Services
Health care personnel will need a medical reporting login credential to access the below documents. If you are a health care provider and would like toRead more
The PA Request Form and. Instructions is posted at MolinaHealthcare.com/OhioProviders under the Forms tab. Medicaid Authorization Reconsideration Process.Read more
DESCRIBE ALL MEDICATION AND ANY SPECIAL DIET THE CHILD RECEIVES AND THE REASON FOR MEDICATION AND SPECIAL DIET. ALL MEDICATIONS A. CHILD RECEIVES SHOULD BERead more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.