Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send form 1051 via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out dhcs 1051 form with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
Click ‘Get Form’ to open the dhcs 1051 form in the editor.
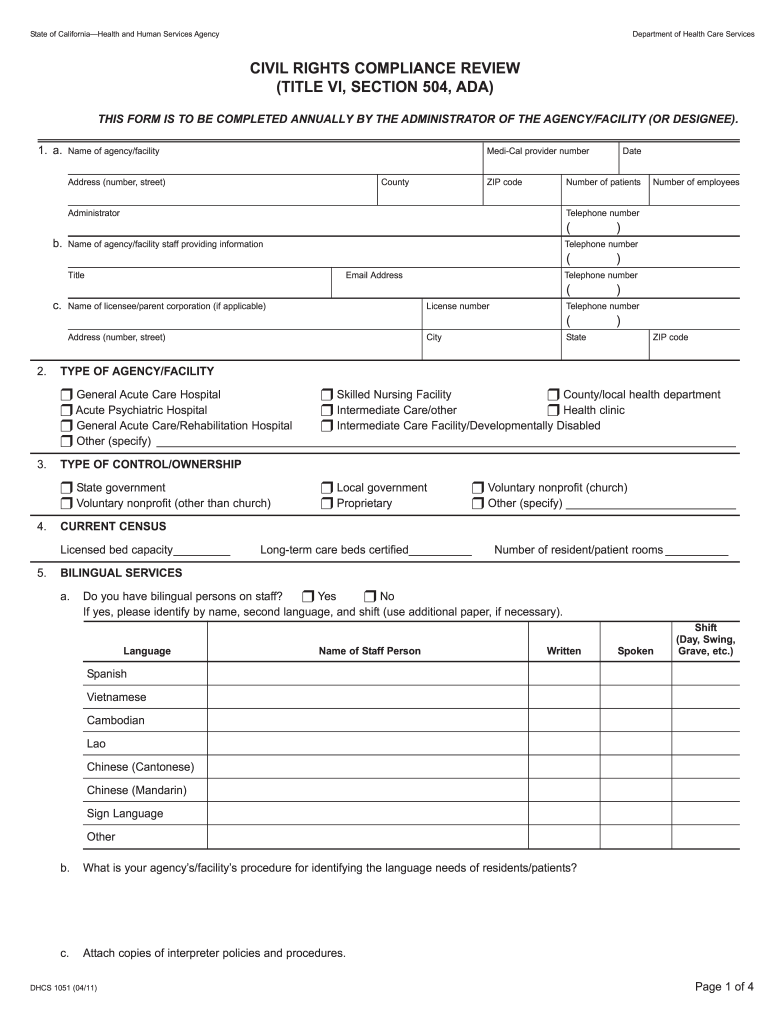
Begin by filling out the agency/facility name, provider number, address, county, ZIP code, and contact details in Section 1. Ensure accuracy as this information is crucial for compliance.
In Section 2, indicate the type of agency/facility by selecting the appropriate checkbox. This helps categorize your facility correctly.
Proceed to Section 3 to specify the type of control/ownership. Choose from options like state government or voluntary nonprofit.
For Section 4, enter your licensed bed capacity and current census data accurately to reflect your facility's capabilities.
Continue through Sections 5 to 14, providing detailed responses about bilingual services, staff composition, resident characteristics, and equal access practices. Use additional paper if necessary for comprehensive answers.
Start using our platform today for free to streamline your form completion process!
Email: CivilRights@dhcs.ca.gov. You may use the ADA Title VI Discrimination Complaint form to submit your complaint to DHCS Office of Civil Rights. The form also contains additional information about your rights. A complaint should be filed as soon as possible or within 180 days of the last act of discrimination.
What is the full form of DHCS in California?
The California Department of Health Care Services (DHCS) is the backbone of Californias health care safety net, helping millions of Californians every day.
What does DHCS do?
DHCS is the single state agency responsible for financing and administering the states Medicaid program, Medi-Cal, which provides health care services to low-income persons and families who meet defined eligibility requirements. Medi-Cal is authorized and funded through a federal-state partnership.
How do I contact CA DHCS?
CMS Net Help Desk Phone: (Toll Free) (866) 685-8449. E-Mail: CMSHelp@dhcs.ca.gov. FAX: (916) 440-5346.
How many days following the resolution must all discrimination grievances be reported to the Department of health care Services?
Discrimination grievances must be submitted to the DHCS Office of Civil Rights within 365 days from the day the discrimination took place. Discrimination grievances may be submitted by filling out the DHCS-1044-DHCS-DISCRIMINATION-COMPLAINT-FORM.
Related Searches
Dhcs 1051 form pdfDhcs 1051 form downloadDhcs 1051 form 2021Dhcs 1051 form onlineDHCS FormsDHCS form 6560State of California Health and Human Services Agency Forms PDFDHCS 6187 form
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
Subcontractor an individual or entity that has a Subcontractor Agreement with the MCP that relates directly or indirectly to the performance of the MCPs obligations under its contract with DHCS.
How do I complain about Medi-Cal in California?
Although DMHC does not review complaints for members in who are not in Knox Keene Plans, you can contact the Department of Health Care Services (DHCS) Medi-Cal Managed Care Office of the Ombudsman. You can call them at 1-888-452-8609 or by email at MMCDOmbudsmanOffice@dhcs.ca.gov.
Related links
Increasing Access to Primary Care Using NPs
by PJ Sandhu 2016 DHCS 1051 (PDF). Required Forms to be certified with Medicaid/Medi-Cal: Application for Medi-Cal Certification as a Primary Care ClinicRead more
civil rights compliance review (title vi, section 504, ada)
THIS FORM IS TO BE COMPLETED BY THE ADMINISTRATOR OF THE AGENCY/FACILITY (OR DESIGNEE). 1. a. Name of agency/facility. Medi-Cal provider number. Date. AddressRead more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.