Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send it via email, link, or fax. You can also download it, export it or print it out.
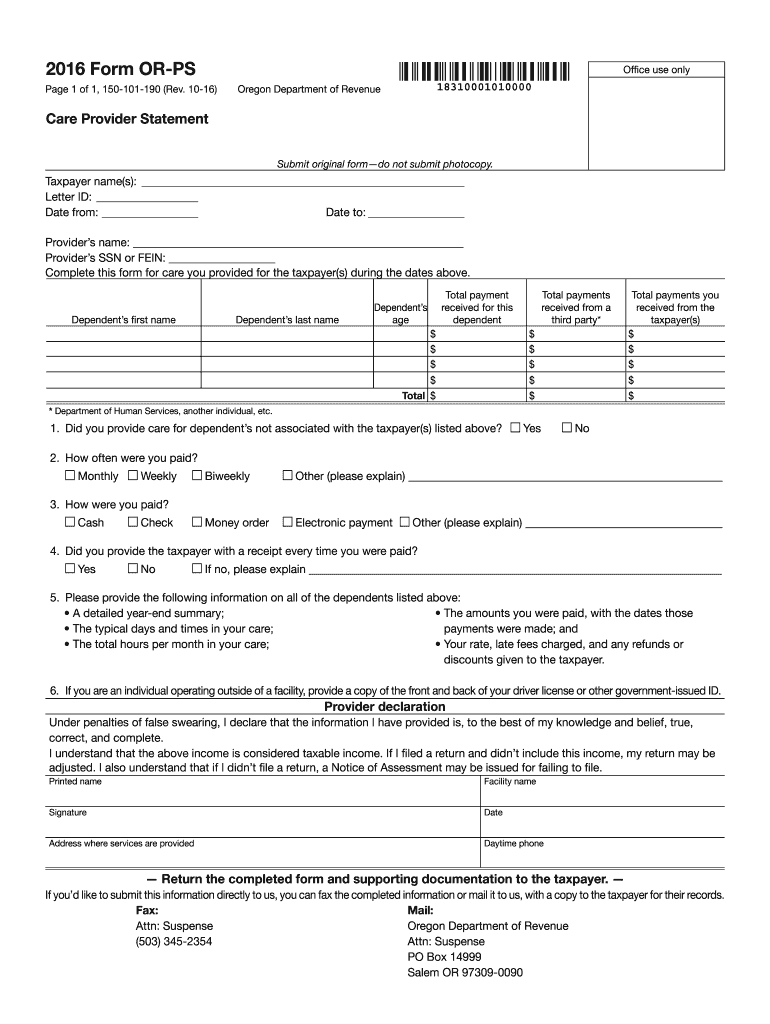
How to use or fill out Form OR-PS, Care Provider Statement, 150-101-190 - Oregon
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
Click ‘Get Form’ to open it in the editor.
Begin by entering the taxpayer's name(s) and Letter ID at the top of the form. If you do not have a Letter ID, input your Social Security number instead.
Fill in the date range for which care was provided, specifying 'Date from' and 'Date to'.
List each dependent's first and last name along with the total payment received for their care. Ensure all amounts are accurately recorded.
Indicate how often you were paid (monthly, weekly, etc.) and specify the payment method used (cash, check, etc.).
Complete the provider declaration section by signing and dating the form. Include your daytime phone number and address where services were provided.
Start using our platform today to easily complete your Care Provider Statement for free!
Fill out Form OR-PS, Care Provider Statement, 150-101-190 - oregon online It's free
See more Form OR-PS, Care Provider Statement, 150-101-190 - oregon versions
We've got more versions of the Form OR-PS, Care Provider Statement, 150-101-190 - oregon form. Select the right Form OR-PS, Care Provider Statement, 150-101-190 - oregon version from the list and start editing it straight away!
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.