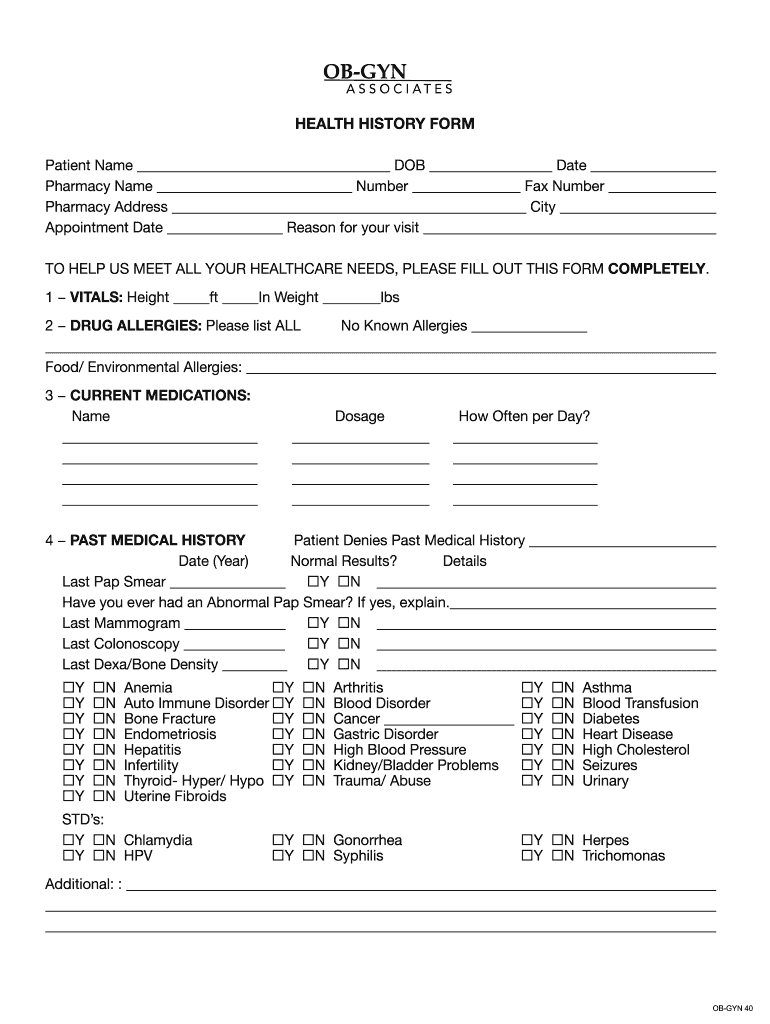



Understanding the OB History Form
The OB history form, commonly known as the obstetrical history form, is a vital document used primarily in prenatal and obstetric care. It collects comprehensive information from patients regarding their reproductive health and previous pregnancies, assisting healthcare providers in creating informed care plans.
Importance of the OB History Form
An accurate obstetrical history is essential for several reasons:
- Provides a detailed overview of a patient's reproductive health, which can influence management and care.
- Helps identify potential risks associated with the patient’s pregnancies, such as preterm labor or gestational diabetes.
- Facilitates communication between healthcare providers, ensuring a holistic understanding of the patient’s medical background.
Key Components of the OB History Form
The ob history form encompasses various elements critical to patient evaluation:
- Personal Information: Basic identification details, including name, date of birth, and contact information.
- Menstrual History: Information regarding the patient’s menstrual cycle, such as the onset of menarche, cycle regularity, and any noteworthy irregularities.
- Obstetric History: Records past pregnancies, including outcomes (live births, miscarriages, stillbirths), complications, and method of delivery (vaginal, cesarean).
- Medical History: Includes chronic conditions, surgeries, and medications, highlighting any health issues that could impact pregnancy.
- Family History: Any genetic or hereditary concerns documented to evaluate risks for pregnancy-related conditions, including congenital anomalies.
Instructions for Completing the OB History Form
Filling out the OB history form requires careful attention to detail. Here are step-by-step guidelines:
- Begin with Personal Information: Accurately fill in your full name, date of birth, and contact information. This identifies you within the healthcare system.
- Detail Menstrual History: Record the age at which your menstruation began, the regularity of cycles, and any menstrual-related health concerns.
- Outline Obstetric History: List each pregnancy chronologically. Specify outcomes and any complications experienced during pregnancies. Include information concerning prenatal care and delivery methods.
- Provide Medical History: Disclose any ongoing medical conditions, past surgeries, and current medications, ensuring to highlight allergies or previous complications during pregnancies.
- Document Family Medical History: Note relevant familial health issues that could impact the pregnancy, including but not limited to diabetes, hypertension, or genetic disorders.
Who Typically Uses the OB History Form
The OB history form is essential for various healthcare professionals involved in obstetric care, including:
- Obstetricians and Gynecologists: Use the form to develop a tailored approach for managing pregnancies and facilitating safe deliveries.
- Nurse Practitioners: Employ information from the form to evaluate patient needs and assist in prenatal counseling.
- Midwives: Utilize detailed obstetrical histories to monitor and manage pregnancy and labor.
- Healthcare Assistants: Sometimes responsible for gathering preliminary information before a patient consultation.
Tips for Preparing Your OB History Form
To ensure that the information gathered is complete and useful:
- Be Thorough: Include as much detail as possible, especially regarding previous pregnancies and any complications faced.
- Review Medical Records: If unsure about specific dates or details, refer to past medical records for accuracy.
- Ask Questions: If confused about any part of the form, don’t hesitate to ask a healthcare provider for clarification.
Additional Considerations for the OB History Form
- Privacy and Confidentiality: Ensure that the information provided on the OB history form remains confidential and is used solely for healthcare purposes.
- Updates: Reassess the form periodically, especially with each new pregnancy, to ensure it reflects the current health status and any changes in medical history.
- Integration into Healthcare: Encourage the use of digital systems for completing and storing OB history forms, which can facilitate easier updates and sharing among healthcare providers.
Variants of the OB History Form
Different versions of the OB history form may exist to cater to specific healthcare practices or patient populations:
- Standard Form: Used for routine obstetric evaluations.
- Specialized Forms: Tailored for high-risk patients or those with specific medical needs.
- Electronic Formats: Digital versions that allow for easy updates and integration with electronic health records.
Understanding the intricacies of the OB history form enhances the effectiveness of prenatal care and improves outcomes for both the mother and the child.