01. Edit your which is the primary purpose of client records online
Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send what is the primary purpose of the client record via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out client care record with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
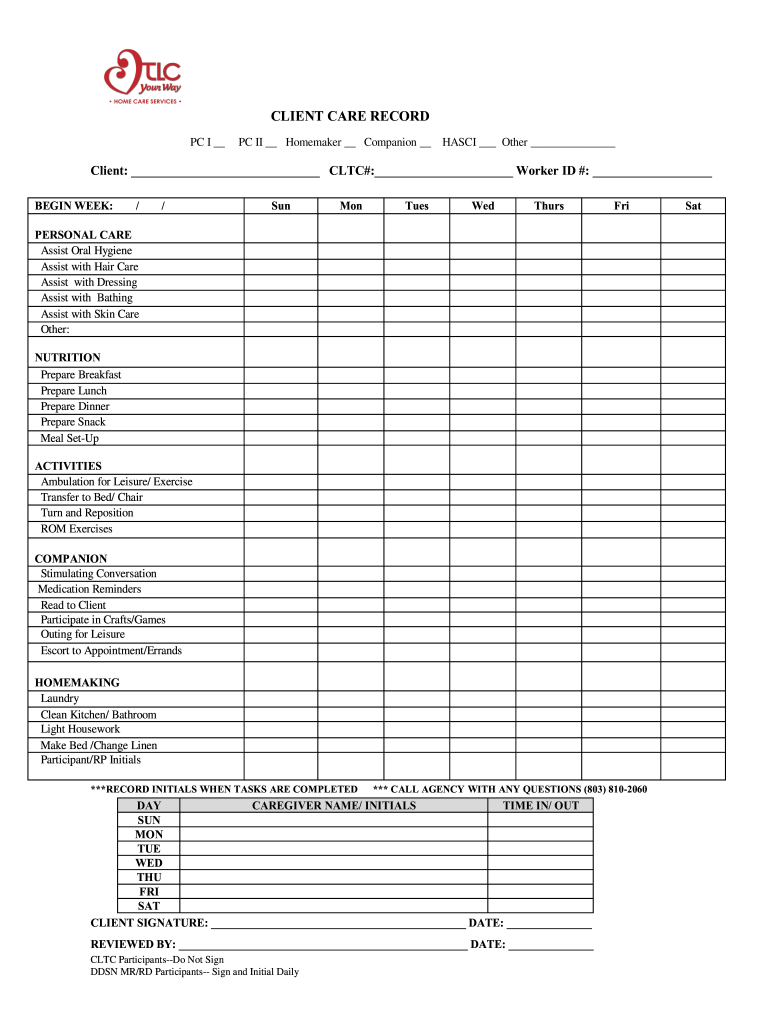
Click ‘Get Form’ to open the client care record in the editor.
Begin by filling in the client’s name and CLTC# at the top of the form. This information is essential for identifying the client.
Select the appropriate services provided by checking the boxes under PC I, PC II, Homemaker, Companion, or HASCI. If other services are provided, specify them in the space provided.
For each day of the week, document caregiver names and initials along with time in/out for accurate tracking of service hours.
In the Personal Care section, mark all tasks that were assisted with during the week. Be sure to include any additional tasks under 'Other' if applicable.
Complete the Nutrition and Activities sections by checking off all relevant tasks performed for meal preparation and engagement activities.
At the end of the form, ensure both client and caregiver signatures are obtained where required. Remember to review all entries for accuracy before finalizing.
Start using our platform today to easily manage your client care records online for free!
athenaClinicals patient record sharing functionality helps you access the patient records you need to achieve the best outcomes for your patients.Read more
Clinical Documentation Best Practices: Ensuring Accuracy
Oct 3, 2025 Clinical documentation best practices: improve accuracy and compliance with clear notes, EHR guidance, correct coding, and audit readiness.
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.