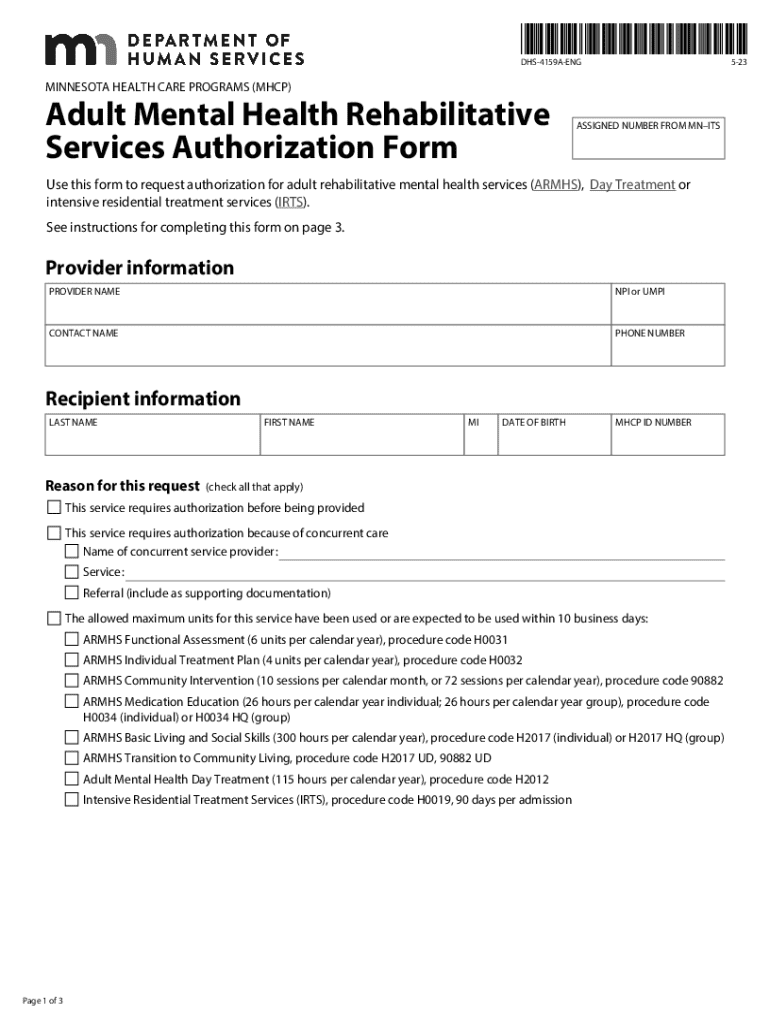



Definition & Purpose of the DHS-4159A-ENG Form
The DHS-4159A-ENG, also known as the Adult Mental Health Rehabilitative Services Authorization Form, is a crucial document used within Minnesota Health Care Programs (MHCP). It serves the purpose of requesting authorization for adult rehabilitative mental health services, such as Adult Rehabilitative Mental Health Services (ARMHS), Day Treatment, or Intensive Residential Treatment Services (IRTS). The form is designed to assess a recipient's eligibility for these services by gathering detailed information about their mental health needs and previous treatment history. This process ensures that individuals receive the appropriate level of care and support based on their specific mental health requirements.
Steps to Complete the DHS-4159A-ENG Form
-
Provider Information: Start by filling in the details of the healthcare provider responsible for overseeing the mental health services. This includes the provider's name, address, and contact information to facilitate communication and verification.
-
Recipient Details: Enter comprehensive information about the person receiving the services. This section should capture the recipient's name, date of birth, and unique identifier within the healthcare system to ensure accurate tracking and record-keeping.
-
Service Request Details: Clearly outline the mental health services needed for the recipient. Provide justification for each service, backing it with evidence from prior assessments or evaluations. Ensure the requested services align with the recipient's mental health goals and treatment plan.
-
Prior Treatment History: Detail the recipient’s previous mental health service engagements. Indicate the types of services provided, the timeframes, and the outcomes. This history aids in crafting a well-informed authorization decision by highlighting patterns or recurring issues.
-
Supporting Documentation: Attach all required supporting documents, such as clinical assessments, treatment plans, and letters from mental health professionals. These documents substantiate the necessity of the proposed services and provide a comprehensive view of the recipient's mental health situation.
-
Provider Signature: The authorized healthcare provider must review all entries and affirm the accuracy and necessity of the requested services. Their signature finalizes the form, confirming the information is accurate and complete.
Who Typically Uses the DHS-4159A-ENG Form
The DHS-4159A-ENG form is primarily utilized by mental health professionals, including psychiatrists, psychologists, and licensed counselors. It’s also used by healthcare administrators responsible for coordinating care. These professionals must ensure that potential recipients' mental health needs are accurately represented and documented to secure the necessary authorizations. Additionally, recipients or their guardians may be involved in the form's completion to provide necessary information or consent.


Key Elements of the DHS-4159A-ENG Form
- Comprehensive Recipient Profiling: Essential for tailor-fitting mental health services.
- Thorough Justification Requirement: Providers must offer a well-founded rationale for requested services.
- Inclusion of Past Treatment Data: Provides context and aids in the decision-making process.
- Essential Supporting Documents: Critical for validating the service request.
Importance of the DHS-4159A-ENG Form
By accurately documenting a recipient's mental health needs and service history, the DHS-4159A-ENG form ensures that individuals get appropriate care that aligns with their specific circumstances. This safeguards recipients from unnecessary treatments while promoting effective use of mental health resources. Comprehensive completion of the form minimizes delays in service authorization, directly benefiting the recipients needing timely interventions.
Eligibility Criteria for Using the Form
Eligibility to use the DHS-4159A-ENG form extends to adult recipients already engaged with Minnesota Health Care Programs and identified as requiring additional mental health services. The form facilitates access to supplementary treatments following clinical assessments that indicate a need beyond standard healthcare provisions. Recipients must belong to the defined demographic of adults needing rehabilitative support for mental health challenges, as specified by MHCP guidelines.
Form Submission Methods
The DHS-4159A-ENG form can be submitted through multiple channels for the provider's convenience:
- Online Submission: Providers can fill out and submit the form electronically via approved MHCP online portals, ensuring faster processing and immediate tracking.
- Mail: Providers may opt to print and mail completed forms to designated MHCP addresses.
- In-Person: Delivery to MHCP offices is also possible, particularly when originals of supporting documents are required for verification.
Legal Use of the DHS-4159A-ENG Form
This form operates within the legal frameworks set by Minnesota state healthcare regulations, ensuring that it aligns with privacy laws and healthcare standards. Legal use involves the protection of sensitive recipient data, limiting access to authorized personnel only. The form’s completion and processing adhere to regulations to safeguard both the recipient's confidentiality and the provider's accountability.