


Definition & Meaning
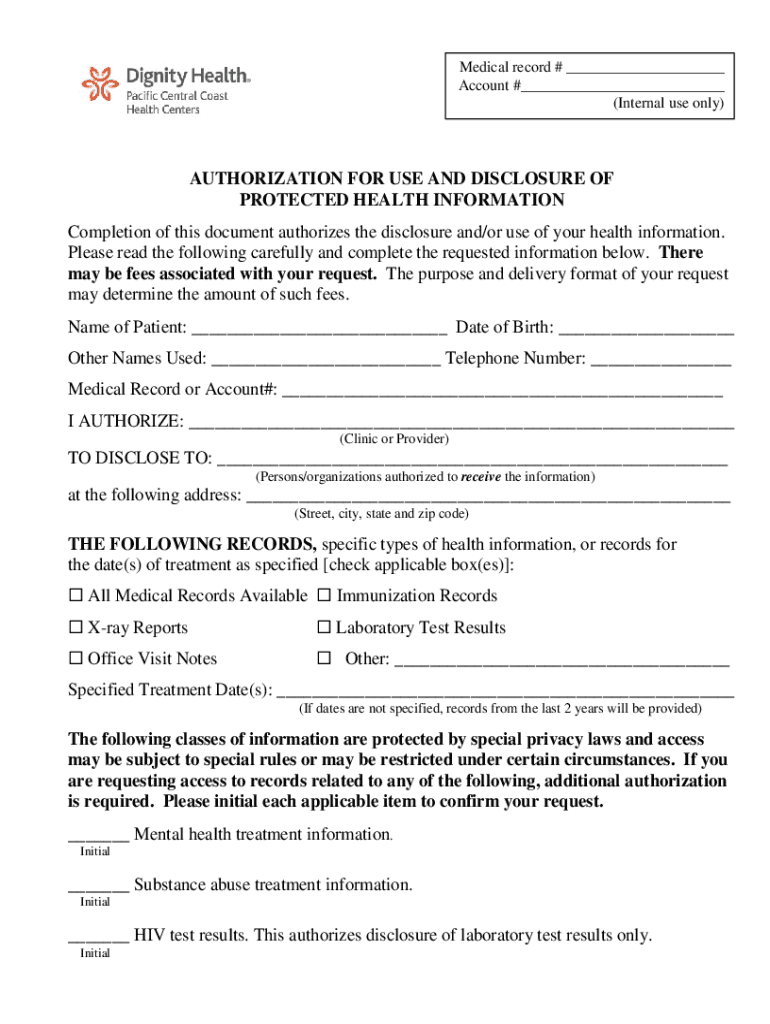
The "Authorization for Use and Disclosure of Protected Health Information" form is a legal document that allows individuals to give healthcare providers permission to release their medical records to specified entities. This process ensures that a patient's private health information (PHI) is shared only with those authorized. The form serves as a communication bridge between patients and healthcare entities, safeguarding sensitive data and ensuring compliance with privacy regulations such as the Health Insurance Portability and Accountability Act (HIPAA).
Key Components of the Form
- Patient Identification: Includes sections for capturing essential details like the patient's name, date of birth, and contact information.
- Recipient Information: Specifies the person or organization authorized to receive the health information.
- Purpose of Disclosure: Outlines why the information is being requested, such as for legal, medical, or personal purposes.
- Types of Information: Details the specific medical records that are to be disclosed, ensuring only necessary information is shared.
How to Use the Form
Using the "Authorization for Use and Disclosure of Protected Health Information" form involves several steps to ensure accurate and secure data handling.
-
Complete Patient and Recipient Details: Clearly fill in the patient's personal information followed by the recipient's details, ensuring there are no errors.
-
Specify Information Types and Purpose: Clearly define what types of medical records are being disclosed and the reason for disclosure.
-
Sign and Date the Form: Both the patient and, if applicable, a legal representative must sign and date the form to validate authorization.
Practical Example
A patient named John Doe wants to transfer his medical records from Hospital A to a specialist at Clinic B. He needs to fill out the authorization form, specifying the specialist's details and the purpose, such as ongoing treatment. John and his legal guardian, if applicable, must then sign and date the form.
Steps to Complete the Form
Completing the "Authorization for Use and Disclosure of Protected Health Information" form requires attention to detail and adherence to specific steps.
-
Review the Form: Start by reading the entire form to understand each section's requirements.
-
Provide Accurate Information: Ensure all patient and recipient information is correct and up-to-date.
-
Detail the Scope of Disclosure: Clearly indicate which medical records are to be shared and the intended use of this information.
-
Sign the Authorization: The patient must sign the form, and if required, a legal guardian or representative's signature is needed.
-
Submit the Form: Follow the healthcare provider's instructions for submission, which may include mail, in-person delivery, or secure online submission.
Why Should You Use the Form
This form is critical for maintaining control over one's personal health information while ensuring that necessary medical data can be shared with authorized parties. It supports seamless transitions of care and compliance with legal standards.
Benefits
- Enhances Communication: Facilitates the transfer of critical medical information between healthcare entities.
- Ensures Security: Complies with HIPAA regulations, preventing unauthorized access to sensitive health data.
- Supports Patient Rights: Allows patients to manage their healthcare decisions and data flow.
Who Typically Uses the Form
Various parties across the healthcare spectrum utilize this form:
- Patients: Individuals seeking to transfer their health records to a new provider.
- Healthcare Providers: Hospitals and clinics that need patient consent to forward medical information.
- Legal Representatives: Guardians or legal proxies for patients who cannot sign the form themselves.


Real-World Use Case
A patient undergoing specialized treatment at an out-of-state facility might use this form to transfer essential medical histories from their primary care provider to the new institution, ensuring comprehensive treatment.
Important Terms Related to the Form
Familiarity with key terminology can aid in understanding and completing the form.
- Protected Health Information (PHI): Any information about health status or healthcare that can be linked to an individual.
- Authorization: Patient's consent to share their health data for specified purposes.
- Disclosure: Act of releasing information.
Legal Use of the Form
The form aligns with legal and regulatory standards, primarily governed by HIPAA. Its use requires strict adherence to legal procedures to validate the transfer of sensitive health data.
Key Legal Considerations
- Privacy Regulations: Ensure compliance with all applicable privacy laws.
- Revocation Rights: Patients have the legal right to revoke authorization at any point.
Key Elements of the Form
Understanding and accurately completing core sections of the form is crucial.
- Patient Information Section: Identifies the individual whose records are being disclosed.
- Recipient Information Section: Clearly defines who will receive the disclosed information.
- Authorization Scope: Specifies what information will be shared and why.
- Patient and Guardian Signatures: Confirms consent with documented acknowledgment.
State-Specific Rules
While this form serves a universal purpose, state regulations may impact its execution.
Considerations for State Compliance
- State Privacy Laws: Some states might have additional privacy requirements beyond HIPAA.
- Format Variations: Adopt different forms or adapt additional sections as per state-specific rules.
Understanding these aspects provides a complete view of the "Authorization for Use and Disclosure of Protected Health Information" form, ensuring its effective utilization.