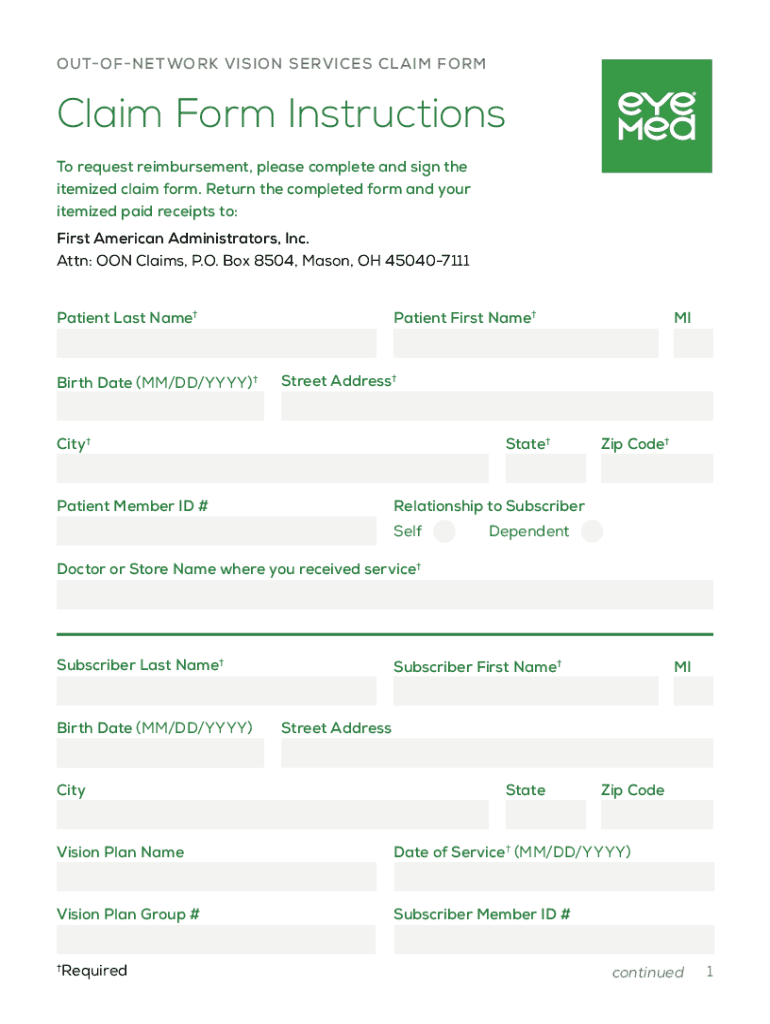
Definition & Meaning
The Eye Med Claim Form is a crucial document used by members of EyeMed Vision Care plans to claim reimbursements for vision services obtained from out-of-network providers. This form is specifically designed to facilitate the processing of claims when services are not accessed through EyeMed's network of participating providers. The form ensures that policyholders can recover the costs or partial expenses associated with vision-related services that are covered under their insurance plan. By meticulously completing the Eye Med Claim Form, members help streamline the processing of their claims, ensuring prompt reimbursement.
How to Obtain the Eye Med Claim Form
To obtain the Eye Med Claim Form, policyholders have several options. It is typically available through the EyeMed Vision Care website, where users can download a digital version of the form to print and fill out manually. Alternatively, members can request a physical copy of the form by contacting EyeMed's customer service department directly via phone or email. Another convenient way is to acquire it through the policyholder's employer or insurance broker, who often have copies readily available for distribution to employees or clients who are part of an EyeMed plan.
Key Elements of the Eye Med Claim Form
The form contains several essential sections that need to be accurately completed to ensure successful processing. Key elements include:
- Member Information: Details like member name, address, and EyeMed ID number.
- Patient Information: The patient’s name and their relationship to the policyholder.
- Provider Information: Contact details and credentials of the out-of-network provider.
- Service Details: A comprehensive list of services rendered, including dates and descriptions.
- Payment Information: Amount paid and the method used for covering these expenses.
Each section must be filled in with precise details to avoid delays in claim processing.
Steps to Complete the Eye Med Claim Form
Completing the Eye Med Claim Form involves several detailed steps to ensure accuracy and completeness:
- Fill Out Member and Patient Sections: Provide personal information for both the policyholder and the individual who received the vision services.
- Input Provider Details: Include the name, address, and contact information of the healthcare provider who delivered the services.
- Specify Service Information: List each service performed along with the date, description, and any applicable procedure codes.
- Attach Itemized Receipts: Securely attach original, itemized payment receipts or billing statements as proof of expenses.
- Review for Accuracy: Double-check all entered details to ensure accuracy and completeness before submission.
- Sign the Form: Ensure that the claim form is signed by the policyholder or patient to validate the information.
Careful adherence to these steps helps in the smooth processing and timely reimbursement of claims.
Required Documents
When submitting the Eye Med Claim Form, individuals must provide certain documents to support their claims:
- Itemized Receipts: Proof of payment for the services provided.
- Billing Statements: Detailed accounts of the services rendered by the healthcare provider.
- Prescription Information: If applicable, a copy of the prescription for vision correction or treatment.
- Insurance Card Copy: Front and back copy of the insurance card to verify coverage details.
Providing these documents ensures that the claim form is fully supported and ready for processing.
Form Submission Methods
The Eye Med Claim Form can be submitted through multiple channels, offering flexibility to the users:
- Mail: Completed forms and accompanying documents can be sent via postal mail to EyeMed’s designated claims address.
- Online Portal: Some policyholders may have access to an online submission portal where digital versions of the form and receipts can be uploaded directly.
- In-Person: For those preferring face-to-face interactions, visiting a local EyeMed office or provider handling claims submissions is an option.
Each method is designed to accommodate different preferences and ensure efficient claim submission.
Penalties for Non-Compliance
Failing to accurately complete or submit the Eye Med Claim Form within required timeframes can lead to several penalties:
- Claim Denial: Incomplete or improperly filled forms may lead to denied claims.
- Delayed Reimbursement: Missing submission deadlines or required documents delays the reimbursement process.
- Financial Loss: Failing to claim within the prescribed window (usually 15 months from the service date) can result in forfeiting reimbursement eligibility.
Understanding these penalties underscores the importance of timely and precise claim submissions to avoid adverse outcomes.
Legal Use of the Eye Med Claim Form
The Eye Med Claim Form is bound by certain legal uses and limitations:
- ESIGN Act Compliance: When forms are electronically submitted, they are subject to electronic signature regulations ensuring authenticity.
- Fraud Prevention: The form includes a section warning against fraudulent claims, highlighting legal consequences for false submissions.
- Privacy Protection: The form and submitted documents are subject to HIPAA regulations, protecting the personal health information of the claimant.
Comprehensive knowledge of these legal entanglements ensures both rightful claim processing and compliance with applicable laws.