Definition & Meaning
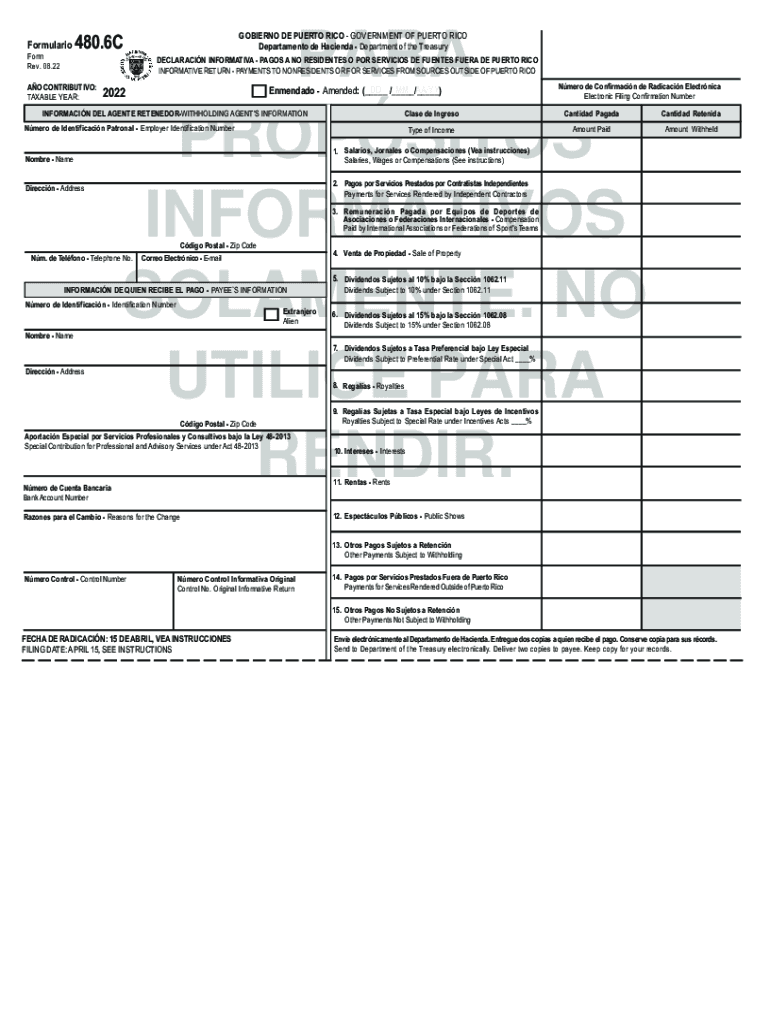
The "Modelo SC 2907 A Form AS 2907 A" is a specific tax form used in Puerto Rico for reports that relate to particular financial obligations or transactions. It is designed to gather detailed information necessary for regulatory and compliance purposes. Understanding the form’s meaning is essential as it guides users on how to correctly report certain financial details to meet state and federal requirements.
Key Aspects of the Form
- Targets financial data related to income, transactions, or withholdings.
- Used primarily by individuals or entities with specific tax reporting needs.
- Ensures compliance with local Puerto Rican tax regulations alongside applicable U.S. standards.
How to Use the Modelo SC 2907 A Form AS 2907 A
The proper filing of the Modelo SC 2907 A Form AS 2907 A requires a thorough understanding of its structure and purpose. It is typically used to report specific kinds of income or transactions as outlined by the Puerto Rico Department of the Treasury.
General Instructions for Use
- Identify Purpose: Determine the reason for filing to ensure the right sections of the form are completed.
- Gather Information: Collect all necessary financial data and documentation before starting.
- Accurate Completion: Follow the form's instructions carefully to avoid common errors in entry fields.
Steps to Complete the Modelo SC 2907 A Form AS 2907 A
Proper completion of the form involves several steps to ensure accuracy and compliance. Each section needs to be filled out with precise attention to detail.
Detailed Steps
-
Header Information:
- Fill in the taxpayer identification number.
- Provide basic contact information.
-
Financial Details:
- Enter specific income or transaction amounts in designated fields.
- Ensure all figures are reported in U.S. dollars unless otherwise specified.
-
Verification:
- Double-check entries for errors.
- Include any required signatures for validation.
Why Should You Use the Modelo SC 2907 A Form AS 2907 A?
Utilizing this form is crucial for individuals or businesses that need to maintain compliance with specific tax obligations in Puerto Rico. It ensures that all financial interactions are properly documented and reported.
Benefits
- Regulatory Compliance: Meets the requirements set by tax authorities.
- Transparent Reporting: Helps in detailing financial transactions clearly to avoid misunderstandings or audits.
- Fiscal Accountability: Assists in keeping comprehensive records for personal or business accounting.
Who Typically Uses the Modelo SC 2907 A Form AS 2907 A
The form is predominantly used by taxpayers who have specific reporting needs within Puerto Rico. This includes a wide array of entities from individual taxpayers to corporate bodies.

Typical Users
- Individual Taxpayers: Those with income that needs to be reported under specific conditions.
- Businesses and Corporations: Organizations operating within or in relation with Puerto Rico’s tax jurisdiction.
- Legal Entities: Partnerships and other legal entities involved in specific types of financial transactions.
Important Terms Related to Modelo SC 2907 A Form AS 2907 A
Understanding key terminology associated with the form enhances the ability to complete it accurately and fully appreciate its implications.
Terms to Know
- Withholding Agent: Individual or entity responsible for withholding tax from payments.
- Gross Income: The total income before any deductions or exemptions.
- Deductions: Amounts that can be legally subtracted from gross income.
Legal Use of the Modelo SC 2907 A Form AS 2907 A
The legal framework surrounding the form dictates its correct usage, ensuring compliance with both Puerto Rican and broader U.S. tax laws.
Regulatory Compliance
- Federal and State Requirements: Aligns with both U.S. federal tax regulations and Puerto Rican legislation.
- Do’s and Don’ts: Users must adhere to set guidelines to avoid penalties or legal implications.
Filing Deadlines / Important Dates
Staying aware of key dates related to the filing of the Modelo SC 2907 A Form AS 2907 A is crucial for timely compliance and to avoid any late submission penalties.
Key Dates
- Annual Filing Date: Must be submitted by the end of the fiscal year, typically on April 15.
- Extension Requests: Procedures available for requesting filing extensions under specific circumstances.
Required Documents
Completing the form often requires the submission of additional documents to verify the information reported and ensure comprehensive compliance.
Essential Documents
- Income Statements: Proof of income relevant to the reporting period.
- Transaction Records: Documentation of financial dealings pertinent to the form’s requirements.
- Identification Proof: Necessary for both individual and corporate filings.
Careful preparation and submission of the Modelo SC 2907 A Form AS 2907 A ensure compliance with tax obligations, helping individuals and businesses avoid potential legal issues or financial penalties.