


Definition and Meaning of the Authorization Form
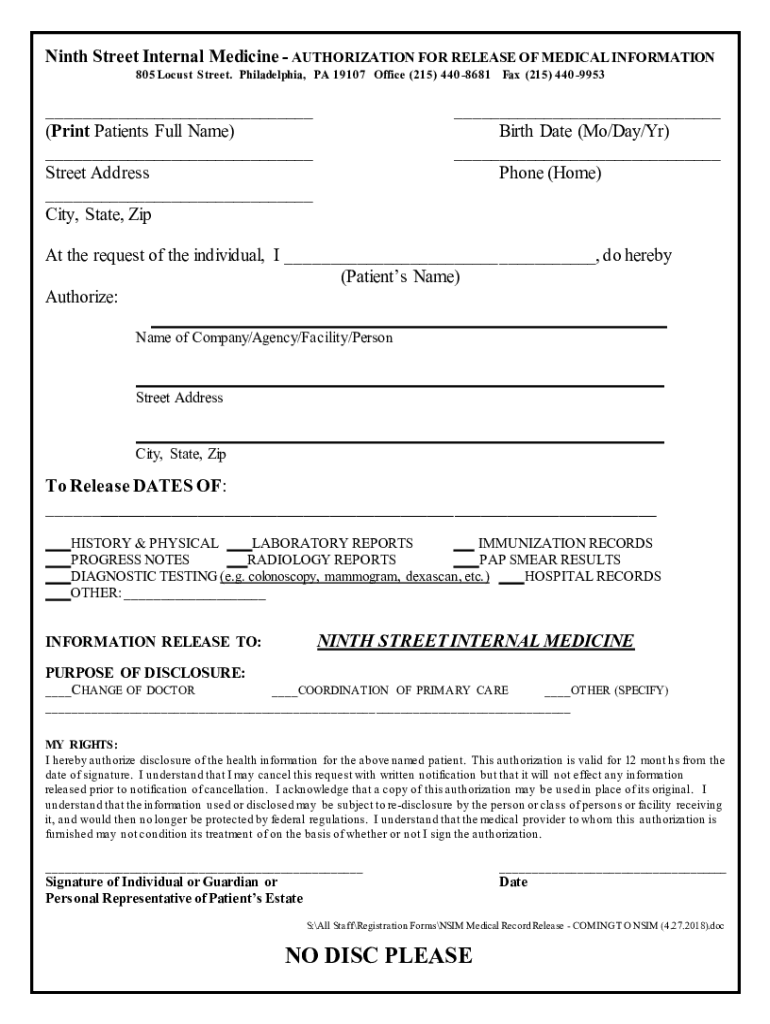
The "Ninth Street Internal Medicine- AUTHORIZATION FOR RELEASE OF" is a legal document utilized by patients to allow Ninth Street Internal Medicine to disclose their medical information to specified individuals or entities. This document is crucial for ensuring that patient data is handled according to legal standards and patient preferences. It outlines which medical records can be shared, the purpose of the disclosure, and the duration of the authorization, which is typically valid for twelve months unless revoked.
Key Elements of the Form
- Patient Details: This section records the patient's personal information, including name and contact details.
- Records to Be Released: Patients specify which medical records can be disclosed, such as test results or treatment history.
- Disclosure Purpose: Defines why the information is being shared, such as for transferring care to another physician or for insurance purposes.
- Patient Rights: Highlights the patient's rights regarding revocation and understanding of the authorization.
How to Use the Authorization Form
Using the "Ninth Street Internal Medicine- AUTHORIZATION FOR RELEASE OF" form involves several essential steps.
- Read Thoroughly: Ensure you understand each section before filling it out. This includes knowing the specific records you wish to release and to whom.
- Accurate Information: Fill in all required fields with precise information to avoid delays.
- Specify the Recipient: Clearly indicate the person or organization authorized to receive your records.
- Purpose Clarification: State the specific reasons for releasing the information, as this defines the scope of the authorization.
- Sign and Date: A signature and date are mandatory to make the form legally binding.
Steps to Complete the Form
Completing the "Ninth Street Internal Medicine- AUTHORIZATION FOR RELEASE OF" involves a systematic approach:
- Obtain the Form: You can get the authorization form directly from Ninth Street Internal Medicine or download it from their official website.
- Provide Personal Information: Include your full name, date of birth, and other identifying information in the designated sections.
- Select Records to Be Released: Specify the types of information you want disclosed, ensuring only relevant records are shared.
- Identify the Recipient: Name the individual or entity that will receive the information.
- Explain the Purpose: Clearly articulate the reasons for the release, whether for continued care or legal purposes.
- Sign the Form: Ensure you sign the document where indicated to validate the authorization.
- Submit the Form: Return the completed form to Ninth Street Internal Medicine for processing.
Legal Use of the Authorization Form
The proper and legal use of the authorization form is critical in maintaining compliance with health privacy laws such as the Health Insurance Portability and Accountability Act (HIPAA). This form ensures that patient information is shared responsibly and only with the patient’s explicit consent. Understanding that this document grants certain access rights to the recipient is paramount, as it impacts both patient privacy and the legal handling of medical data.
Why Is It Important?
Signing the "Ninth Street Internal Medicine- AUTHORIZATION FOR RELEASE OF" is significant for a variety of reasons:
- Continuity of Care: Enables seamless transition of care by allowing new healthcare providers access to essential medical history.
- Insurance Claims: Assists in processing insurance claims where medical history or specific diagnosis information is required.
- Legal Documentation: Provides necessary evidence in legal situations where medical conditions are relevant.
- Patient Empowerment: Enhances patient control over personal health information, ensuring it is shared only with trusted parties.
Who Typically Uses the Authorization Form?
The "Ninth Street Internal Medicine- AUTHORIZATION FOR RELEASE OF" is widely used by:
- Patients seeking to transfer their medical records to other healthcare providers.
- Healthcare Providers who require patient consent to access or share medical records.
- Legal Representatives in cases where medical documentation is required by law.
- Insurance Companies needing access to records for claims processing.

Important Terms Related to the Form
Understanding specific legal and medical terminology enhances clarity while filling out the form:
- HIPAA: Refers to the federal law that protects sensitive patient health information.
- Revocation: The formal withdrawal of authorization by the patient, which stops further disclosure.
- Scope of Disclosure: Defines the extent and limitations of shared information outlined in the form.
- Electronic Health Records (EHR): Digital version of a patient's paper chart, often involved in record-sharing processes.
Examples of Using the Authorization Form
Consider real-world scenarios that highlight the application of this form:
- For Students: A college student moving out of state might authorize their new physician to access past medical records from Ninth Street Internal Medicine.
- For Job Relocation: An employee relocating for work may need to authorize information release to a new healthcare provider in a different city.
- Legal Cases: Patients involved in legal matters may need to share certain health information, necessitating clear and documented authorization.
Each of these use cases underscores the versatility and necessity of this form across various life situations.