Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send nyc hcfsa claim form 2024 via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out hcfsa claim form with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
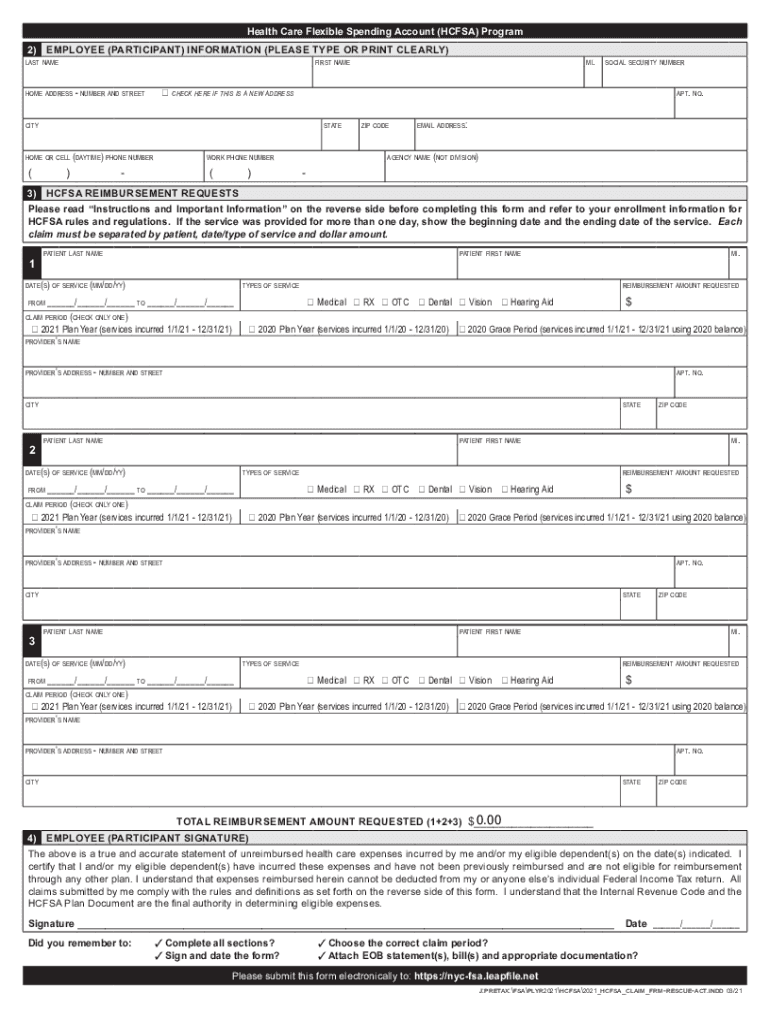
Click ‘Get Form’ to open the HCFSA claim form in the editor.
Begin by filling out your personal information in the EMPLOYEE (PARTICIPANT) INFORMATION section. Ensure you type or print clearly your last name, first name, home address, phone number, and email address.
In the HCFSA REIMBURSEMENT REQUESTS section, list each patient’s last name and the dates of service. Specify the type of service provided and check the appropriate claim period box.
For each service, enter the provider's name and address along with the reimbursement amount requested. Make sure to separate claims by patient and date/type of service.
Finally, sign and date the form in the EMPLOYEE (PARTICIPANT SIGNATURE) section. Double-check that all sections are completed and that you have attached any necessary documentation before submitting.
Start using our platform today for free to streamline your HCFSA claim process!
HCFSA REIMBURSEMENT REQUESTS. Each claim must be separated by patient, date/type of service and dollar amount. The minimum reimbursement amount requested must
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.