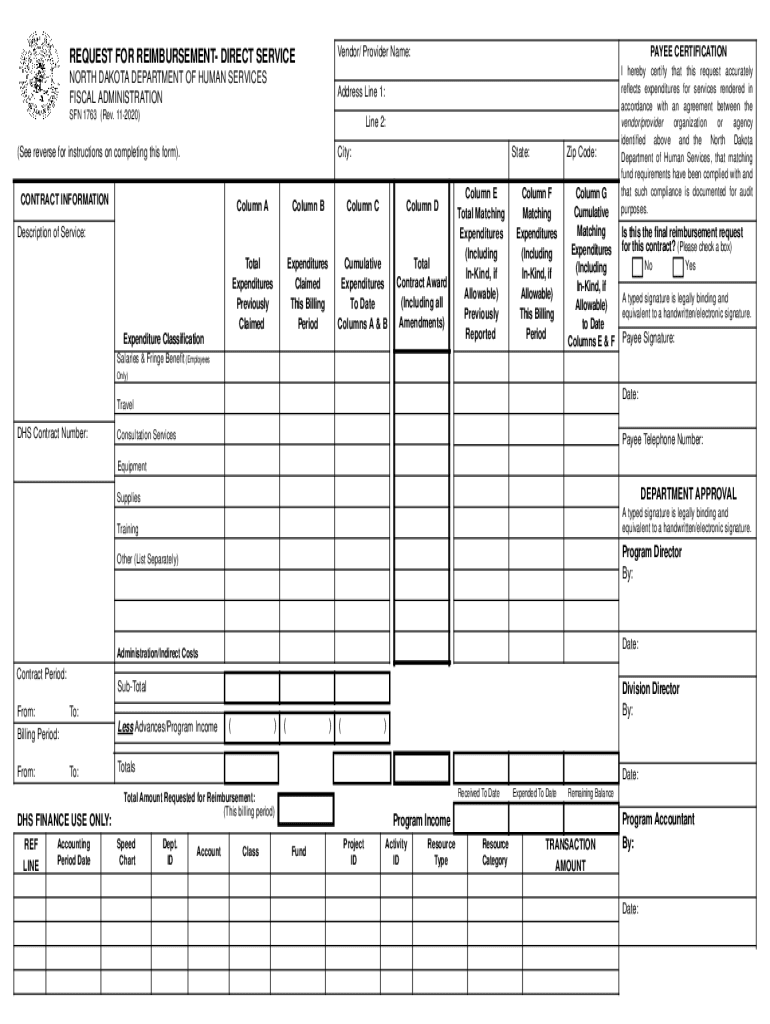
Start using our platform today for free to streamline your SFN 1763 completion!
Sure, a typed name is recognized as a legitimate electronic signature when you create it on your paperwork utilizing a compliant solution like DocHub. Simply upload your sfn 1763 to our editor, click Sign in the top tool pane → Create your signature → Type your name in the appropriate tab, and decide how it will look on your document.
You need only a web connection and a browser to complete your sfn 1763 on an iOS phone. Open the DocHub website and authenticate. Then, add your document or choose it from the list in your dashboard. Then use our editing instruments to complete your form and preserve all your changes. You can also send it to a dedicated recipient right away.
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
Learn more