Definition and Overview of the PACU Nurse Report Sheet
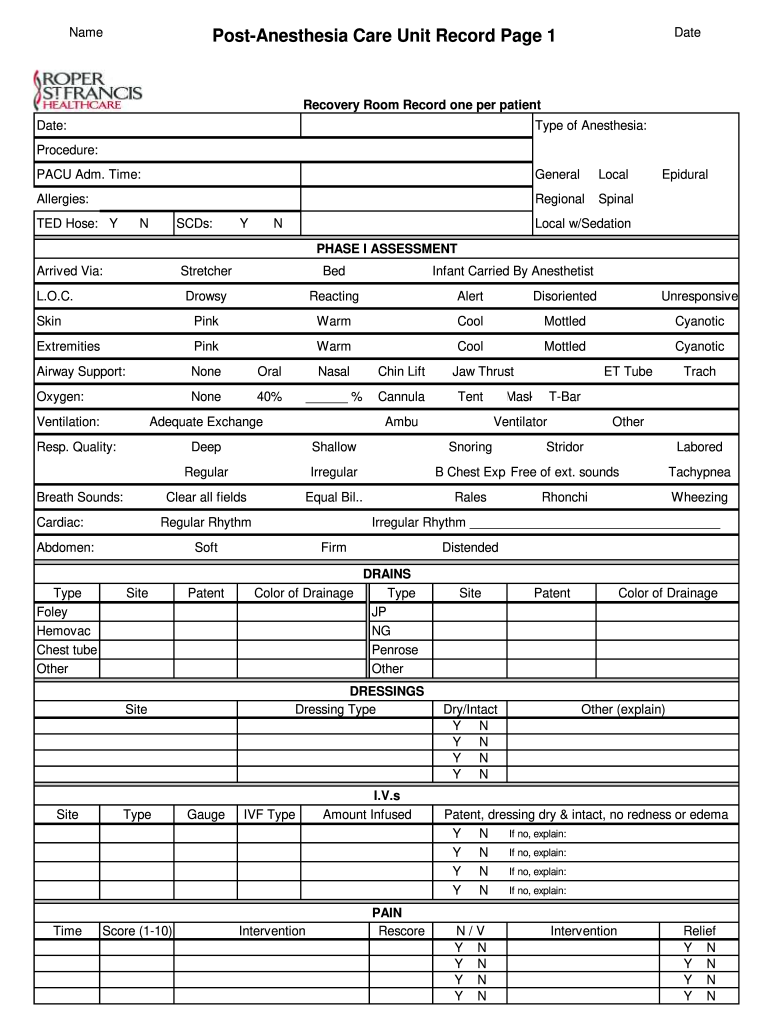
The PACU nurse report sheet is a specialized tool used by nurses in the Post-Anesthesia Care Unit (PACU) to document and monitor patients recovering from anesthesia. This structured form is essential for ensuring continuity of care and comprehensive documentation, allowing nurses to track vital information relevant to the patient's recovery process. It includes crucial fields for recording patient data, anesthesia details, vital signs, consciousness levels, and medication administration.
Key Components of the PACU Nurse Report Sheet
The PACU nurse report sheet typically includes the following sections:
- Patient Information: This section captures basic demographics, including the patient's name, date of birth, medical record number, and the attending physician.
- Anesthesia Details: Nurses document the type of anesthesia administered, the duration of anesthesia, and any intraoperative complications that may have occurred.
- Vital Signs Monitoring: Regular assessment of vital signs such as blood pressure, heart rate, respiratory rate, and oxygen saturation is essential. The report sheet facilitates recording these measurements at scheduled intervals.
- Consciousness and Neurological Status: Nurses assess the patient's level of consciousness using standardized scales, which can include the Aldrete scoring system, to ensure that patients meet discharge criteria.
- Pain Management: Documentation of pain levels and analgesic administration helps provide optimal pain control and adjust medications as necessary.
How to Use the PACU Nurse Report Sheet
To effectively utilize the PACU nurse report sheet, nurses should follow a structured approach:
- Initiate Documentation: Begin recording immediately upon patient admission to the PACU. Accurate initial assessments are crucial for shaping ongoing care.
- Systematic Monitoring: Regularly monitor the patient's vital signs and neurological status, documenting findings on the report sheet. This approach promotes timely interventions in response to patient needs.
- Effective Communication: Use the report sheet as a communication tool among healthcare staff. Ensure that all entries are clear and concise to facilitate efficient transfer of information.
- Note Changes in Condition: Document any significant changes in the patient's condition, including sudden dips in vital signs or changes in consciousness levels, as these warrant immediate medical attention.
- Coordinate Discharge Planning: When the patient is stable and meets discharge criteria, use the information documented on the report sheet to guide discharge planning, ensuring all necessary follow-up instructions and referrals are provided.
Steps to Complete the PACU Nurse Report Sheet
Completing the PACU nurse report sheet involves several critical steps:
- Preparation: Ensure that the report sheet is clean and ready for use before patient admission.
- Patient Admission Entry: Fill in the patient's identifying information, including their name and medical record number, as soon as they arrive in the PACU.
- Document Anesthesia Information: Record the type of anesthesia and any relevant details from the surgery or procedure immediately after it concludes.
- Monitor and Record Vital Signs: Measure and document vital signs at regular intervals, such as every five or ten minutes, depending on institutional protocols.
- Assess and Document Consciousness Levels: Use clear language to describe the patient's consciousness and responsiveness throughout their stay in the PACU.
- Pain Assessment and Management: Engage with the patient about their pain levels and record any medication administered, including dosages and times.
- Finalize Documentation: Once the patient is ready for discharge, ensure that all fields on the report sheet are completed appropriately. Double-check for accuracy before submitting to the medical record.
Examples of Using the PACU Nurse Report Sheet
Practical applications of the PACU nurse report sheet highlight its significance in patient care:
- Case Study A: A patient undergoing outpatient knee arthroscopy. Upon admission, the PACU nurse notes the patient's surgical details and anesthesia type. Vital signs are recorded every five minutes, indicating slight hypotension. The nurse adjusts the IV fluids per protocol and documents the intervention.
- Case Study B: A patient recovering from general anesthesia after a cholecystectomy. The PACU nurse uses the report sheet to note fluctuating oxygen saturation levels, triggering additional respiratory support per the anesthesiologist’s orders, ensuring patient safety.
Important Terms Related to the PACU Nurse Report Sheet
Understanding key terminology associated with the PACU nurse report sheet is critical for effective usage:
- Aldrete Score: A scoring system used to assess a patient’s readiness for discharge from the PACU based on criteria such as activity, respiration, circulation, consciousness, and oxygen saturation.
- Post-Anesthesia Care Unit (PACU): The specialized unit within a healthcare facility where patients recover from anesthesia following surgical procedures.
- Vital Signs: Measurements that indicate the physiological status of a patient, such as heart rate, blood pressure, respiratory rate, and temperature.
This terminology facilitates clear communication and comprehension among healthcare professionals using the PACU nurse report sheet, ensuring that critical information is captured and elucidated.