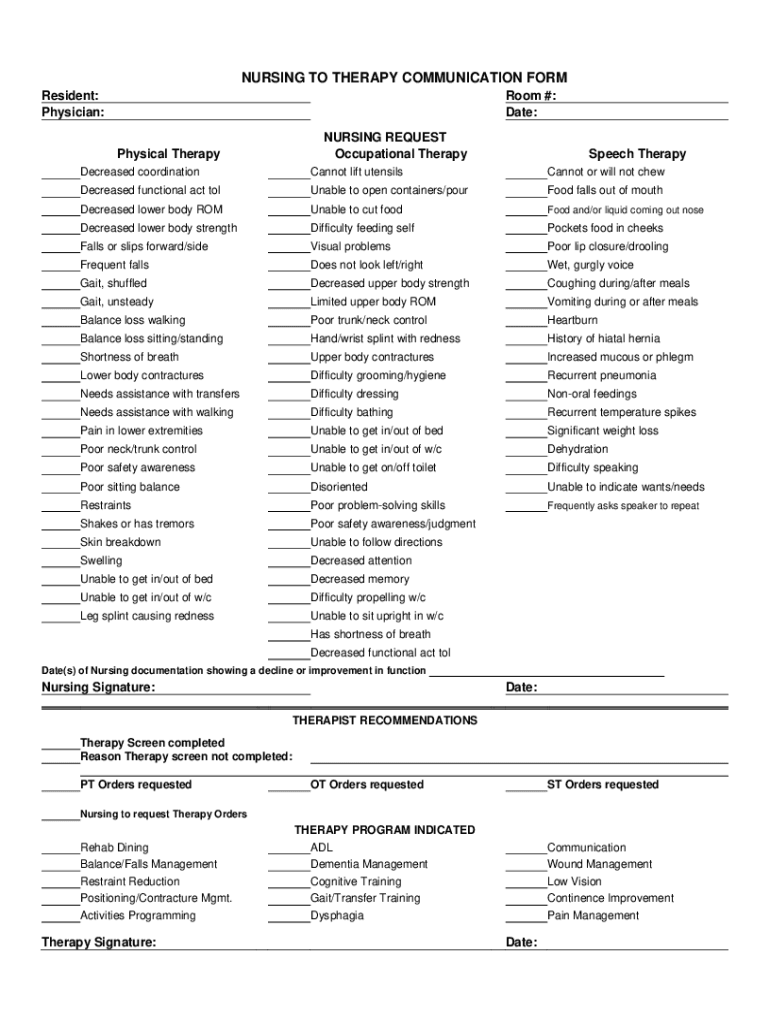



Definition and Meaning of the Nursing to Therapy Communication Form
The Nursing to Therapy Communication Form is a specialized document designed to facilitate effective communication between nursing staff and therapy professionals in healthcare settings. It is integral in ensuring that relevant patient information is shared accurately and promptly, streamlining care coordination. The form acts as a liaison tool, outlining specific therapy needs and instructions related to the resident's care plan, thus enhancing the overall quality of patient care.
Purpose and Objectives
- To communicate specific therapy needs from nursing staff to therapists.
- To record and track patient progress and modifications in therapy protocols.
- To improve coordination and continuity of care within healthcare teams.
Use in Healthcare Settings
The form is commonly used in hospitals, rehabilitation centers, and long-term care facilities where patients receive multifaceted care involving both nursing and therapy services.
How to Use the Nursing to Therapy Communication Form
Completing the Form
To use the form effectively, one must understand the critical sections to be filled:
- Patient Information: Includes name, physician, and room number. This ensures that the document is accurately attributed to the correct resident.
- Therapy Requests: Specifies the types of therapies required, such as occupational, thermophysical, or speech therapy, and details like the decreased coordination or difficulty using utensils.
Submission Process
The completed form should be submitted to the relevant therapy department promptly to avoid any delay in care coordination. It is typically reviewed and then incorporated into the patient’s therapeutic regimen.
Steps to Complete the Nursing to Therapy Communication Form
- Gather Necessary Information: Start by collecting patient-specific data, such as medical history, ongoing treatments, and any unique needs or challenges.
- Fill Out Patient Details: Accurately record the patient’s name, physician, and room number to ensure proper identification.
- Specify Therapy Requirements: Clearly outline the specific therapies needed. Provide detailed descriptions of the issues to be addressed, such as coordination problems or utensil handling difficulties.
- Sign and Date the Form: Ensure the form is signed by the responsible nursing staff and dated for record-keeping and tracking purposes.
Key Elements of the Nursing to Therapy Communication Form
Patient Information Section
- Resident Details: Name, physician, and room number are critical for identification.
- Date of Issuance: Important for tracking and follows up on therapy interventions.
Therapy Needs Section
- Therapeutic Interventions: Lists types of therapy required and specific challenges observed.
- Nursing Observations: Includes comments on patient needs and expected outcomes.
Communication and Coordination
- Facilitates interaction between nurses and therapists.
- Ensures timely updates on patient conditions and therapy progress.
Who Typically Uses the Nursing to Therapy Communication Form
Primary Users
- Nursing Staff: Utilize the form to communicate therapy needs and observations about the patient.
- Therapists: Rely on the form to devise and adjust therapy plans according to communicated needs.
Supporting Roles
- Medical Administrators: Oversee the process, ensuring that the form is properly utilized and integrated into patient records.
- Care Coordinators: Use the form to ensure cohesive care planning and delivery.
Legal Use and Compliance
Compliance Requirements
The use of the Nursing to Therapy Communication Form must comply with healthcare regulations and standards, including patient confidentiality as outlined by guidelines such as HIPAA in the United States. Proper documentation is essential to ensure legal integrity and accountability in patient care.
Impact on Patient Care
Using the form in compliance with legal standards improves patient outcomes by promoting clear communication and avoiding misunderstandings in therapy orders.
Examples of Using the Nursing to Therapy Communication Form
Scenario 1: Acute Care Setting
In an acute care hospital, a patient post-operative care team uses the form to communicate between nursing and physical therapy departments to set rehab goals.
Scenario 2: Long-Term Care Facility
In long-term care, the form is used to adjust a resident’s therapy regimen based on observed changes in physical or cognitive abilities, fostering tailored therapeutic interventions.
Digital vs. Paper Version
Comparison
- Digital Version: Offers real-time updates, easy sharing, and integration with electronic health records (EHRs). It is often accessible across various devices, increasing workflow efficiency.
- Paper Version: Preferred in facilities where digital infrastructure is limited or for immediate physical documentation needs.
Benefits
- Digital forms enhance accuracy through automated data entry and reduce risks of loss associated with paper forms.
These sections combine practical guidance and detailed content, meeting the requirement for comprehensive coverage of the "Nursing to Therapy Communication Form."