


Definition and Purpose of the Mississippi State Prior Authorization Request Form
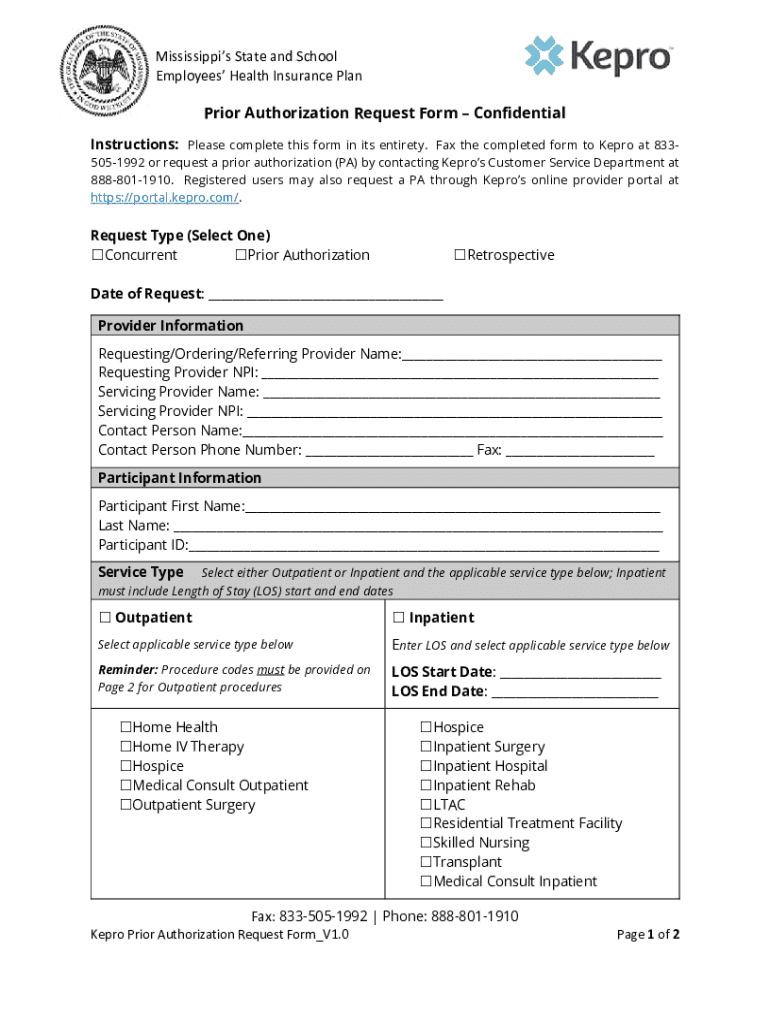
The Mississippi State Prior Authorization Request Form, officially known as the Caremark MississippiPARequestFormMississippi, is an essential document for healthcare providers seeking approval from the State and School Employees' Health Insurance Plan to proceed with certain medical services. It is a formal application that seeks authorization for care and services, thereby ensuring both compliance with insurance requirements and appropriateness of the treatment offered.
- Purpose: The primary goal is to confirm that the medical services align with the insurance policy guidelines and are deemed necessary for the patient involved. This document prevents unauthorized claims, minimizes unwarranted expenses, and ensures patients receive appropriate care.
- Utilization: Healthcare professionals use this form when procedural services outlined by the state insurance require pre-approval. It avoids lapses in coverage due to unauthorized procedures.
How to Use the Mississippi Prior Authorization Request Form
Using the Mississippi Prior Authorization Request Form correctly is crucial for securing the necessary permissions without delay.
- Obtain the Form: Secure the form from relevant online health insurance portals, healthcare provider facilities, or state insurance administrators.
- Complete Provider Details: Include complete information of the healthcare provider, such as name, contact details, and healthcare identifier numbers.
- Patient Information Section: Fill out patient’s name, insurance number, health plan details, and comprehensive contact information.
- Service Description: Clearly indicate the medical services requested, specifying outpatient, inpatient, or other specialized services to determine coverage.
- Diagnosis Information: Record the patient’s diagnosis, ensuring compatibility with requested services for verification against plan requirements.
- Submission: Submit the completed form through the appropriate channels, such as online submission portals, email, or physical mail, depending on the options made available by the state insurance body.
Steps to Complete the Prior Authorization Request Form
Completing the Caremark MississippiPARequestFormMississippi State Prior Authorization Request Form involves several methodical steps to ensure all necessary information is accurately provided.
- Detail Entry: Begin by entering the healthcare provider's information and verifying its accuracy.
- Patient Identification: Enlist the patient’s identifying details, ensuring you have the most current information.
- Documentation of Service Requirements: Note the specific medical services for which approval is sought, clarifying their urgency and necessity.
- Diagnosis Report: Attach a diagnosis report or relevant medical findings that support the need for proposed treatments.
- Signature: The provider must sign the form, authenticating the request and avowing that all listed information is genuine and required.
- Verification: Double-check the entries for completeness and accuracy to prevent processing delays.
Key Elements of the Prior Authorization Request Form
Understanding the components of the form helps streamline its completion process, reducing processing time and improving approval rates.
- Provider Information: Elements include provider ID, contact information, and service facility.
- Patient Identification: Consists of full name, date of birth, insurance details, and health plan ID.
- Service Details: Specific data on requested medical services, including anticipated dates and procedural codes.
- Diagnosis Information: Medical codes and notes that outline the patient's condition.
- Authorization and Agreement: Section for provider's signature and any additional stipulations required by the insurance plan to validate the form.
Required Documents for Submission
To ensure successful processing of the Mississippi State Prior Authorization Form, have the following documents ready for attachment during submission:
- Doctor’s Referral or Recommendation: Providing context and justification for each medical service requested.
- Patient’s Medical Records: Including recent diagnostics related to the requested procedures.
- Insurance Details: A copy of the patient's current insurance policy or cards to confirm coverage limits.
- Supporting Evidence: Any supplementary documentation, such as lab results or historical data, supporting the necessity of the service.
Who Typically Uses the Prior Authorization Request Form
The Prior Authorization Request Form is primarily used by:
- Healthcare Providers: To gain pre-approval for procedures requiring insurance verification.
- Insurance Administrators: For evaluating the appropriateness and need for requested services under specific policies.
- Patients: Indirect users benefiting by receiving services that are pre-authorized and covered under their insurance plan.

Legal Use and Compliance
Fulfilling legal obligations, the Mississippi State Prior Authorization Request Form is designed with compliance in mind, ensuring all requested services are thoroughly vetted for necessity before approval.
- Regulatory Compliance: Aligns with healthcare regulations to ensure justification for services against insurance guidelines.
- Patient Protection: Protects patients from unexpected medical costs due to unapproved claims.
- Data Integrity: Ensures secure handling of sensitive patient information according to applicable laws and standards.
State-Specific Rules for Submission
State-specific regulations govern the submission and approval procedures of the Prior Authorization Request Form, ensuring consistency with Mississippi’s health insurance laws.
- Submission Channels: Depending on the state mandates, choose from digital or paper submissions.
- Review Timelines: Adherence to specific state timelines for form approval is essential for timely service provision.
- State Amendments: Be aware of any state-specific legislation changes impacting the authorization process.
By following these steps, regulations, and guidelines, users can effectively navigate the Caremark MississippiPARequestFormMississippi State Prior Authorization Request Form process, ensuring proper healthcare service delivery within the legal framework.