


Definition and Purpose of the Child & Adolescent Health Examination Form
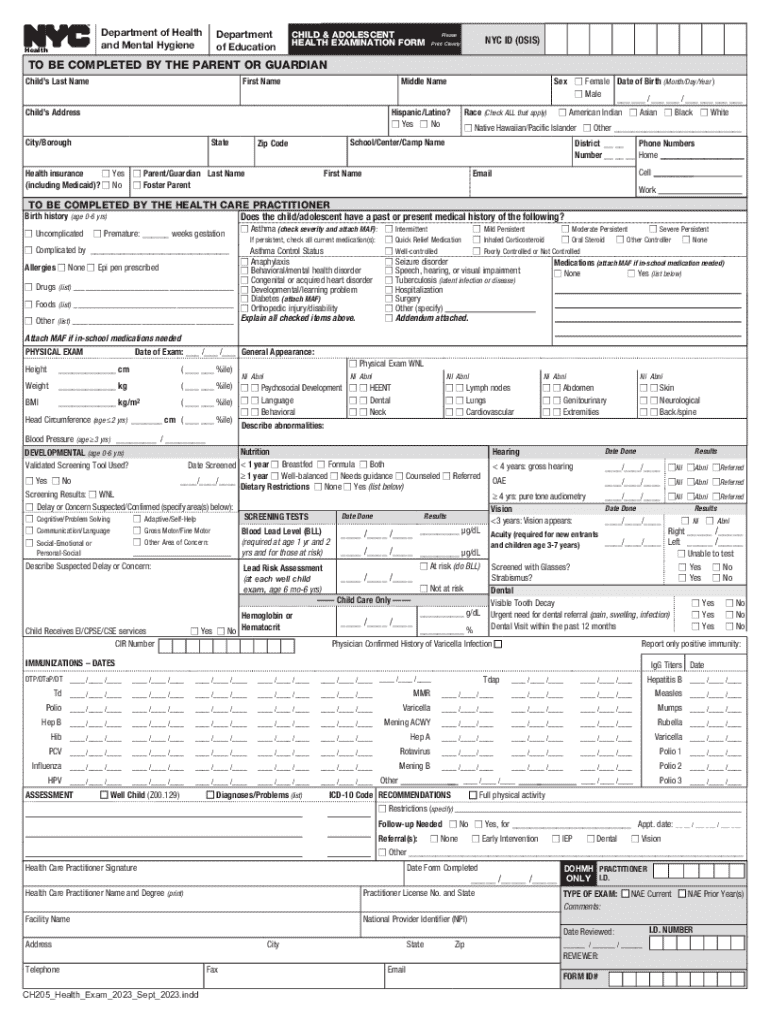
The Child & Adolescent Health Examination Form, known as the CH205, is a detailed document used by the Department of Health and Mental Hygiene and the Department of Education to gather vital health information about children and adolescents. This form serves as an official record of a child's medical history, physical examination results, developmental screenings, and immunization records. It helps ensure that children meet the necessary health standards for school enrollment and continued attendance, as well as facilitating early detection of potential health issues.
Essential Information Collected
The CH205 requires comprehensive details such as:
- Personal demographics: Name, birthdate, and school information.
- Medical history: Previous illnesses, allergies, and surgeries.
- Physical examination: Vital signs, vision, and hearing test results.
- Developmental screenings: Milestones measured against age norms.
- Immunization records: Documentation of all vaccines administered.
- Recommendations: Any required follow-up care or referrals.
This extensive data collection is aimed at promoting the health and safety of students within the school environment.
How to Obtain the CH205 Form
The CH205 form can be accessed through various official channels:
- State Health Department: Most health departments provide this form online, often allowing for direct download.
- Department of Education Websites: Schools may require the form for enrolment, linking to it on their websites.
- Healthcare Providers: Pediatricians and family clinics usually have copies on hand and can provide them during appointments.
Online Accessibility
To obtain the form electronically:
- Visit your state’s health department website.
- Download the form directly to your computer or mobile device.
- Print the form if a paper version is needed for submission.
Steps to Complete the CH205 Form
Filling out the CH205 form requires detailed input from both parents and healthcare providers. Here are the steps:
- Parent/Guardian Section: Complete the child’s personal details and medical history.
- Healthcare Provider Section:
- Conduct a thorough physical examination and document results.
- Record results from developmental screenings.
- Update and verify immunization records.
- Review and Sign: Both the parent/guardian and healthcare provider must review and sign the form to validate the information provided.
Common Pitfalls
- Inaccurate or incomplete information may cause delays.
- Ensure signatures are correctly placed and dated.
Why Use the CH205 Form
The CH205 form is essential for several reasons:
- School Admission: Many schools mandate the form for ensuring student health preparedness.
- Health Monitoring: Regular updates help track child health developments.
- Compliance: It ensures adherence to state health laws and regulations, preventing outbreaks of communicable diseases in schools.
Benefits
- Early Detection: Identifies potential health issues before they become severe.
- Comprehensive Care: Encourages dialogue between healthcare providers and educators about individual needs.
Who Typically Uses the CH205 Form
The CH205 form is predominantly used by:
- Parents and Guardians: To ensure their children meet school health requirements.
- Pediatricians and Nurses: For conducting thorough health assessments and completing the form's medical sections.
- School Administrators: To verify that enrolment criteria are met.


Strategic Usage
This form supports collaboration across healthcare and educational sectors, fostering a comprehensive approach to childhood health management.
Key Elements of the CH205 Form
The form is comprised of several critical sections:
- Demographics: Basic information necessary for record-keeping.
- Health Screenings: Sections capturing physical exam results and developmental progress.
- Immunization Tracking: Ensuring compliance with state vaccine mandates.
- Medical Recommendations: Providing actionable next steps for identified health issues.
Detailed Components
Each part of the form is crucial for providing a holistic view of a child’s health, facilitating targeted interventions when needed.
Legal Considerations and State-Specific Rules
The CH205 form complies with U.S. health regulations and varies by state:
- Immunization Requirements: States may have distinct vaccine requirements.
- Submission Protocols: Methods of submission and deadlines can differ.
Important Legal Points
- Confidentiality: Adherence to HIPAA ensures the protection of children’s health information.
- State Laws: Awareness of state-specific health laws is critical for proper completion and submission.
Digital Versus Paper Versions
Both digital and paper versions of the CH205 form are available, each with distinct advantages:
- Digital Version: Offers ease of storage and transmission.
- Paper Version: Preferred for face-to-face consultations and immediate verification.
Choosing the Right Format
The decision often depends on personal convenience and institutional requirements, with digital versions supporting environmentally friendly practices.
By understanding and utilizing the CH205 form effectively, all parties involved can ensure a proactive approach to managing child and adolescent health needs within the educational system.