Definition & Meaning
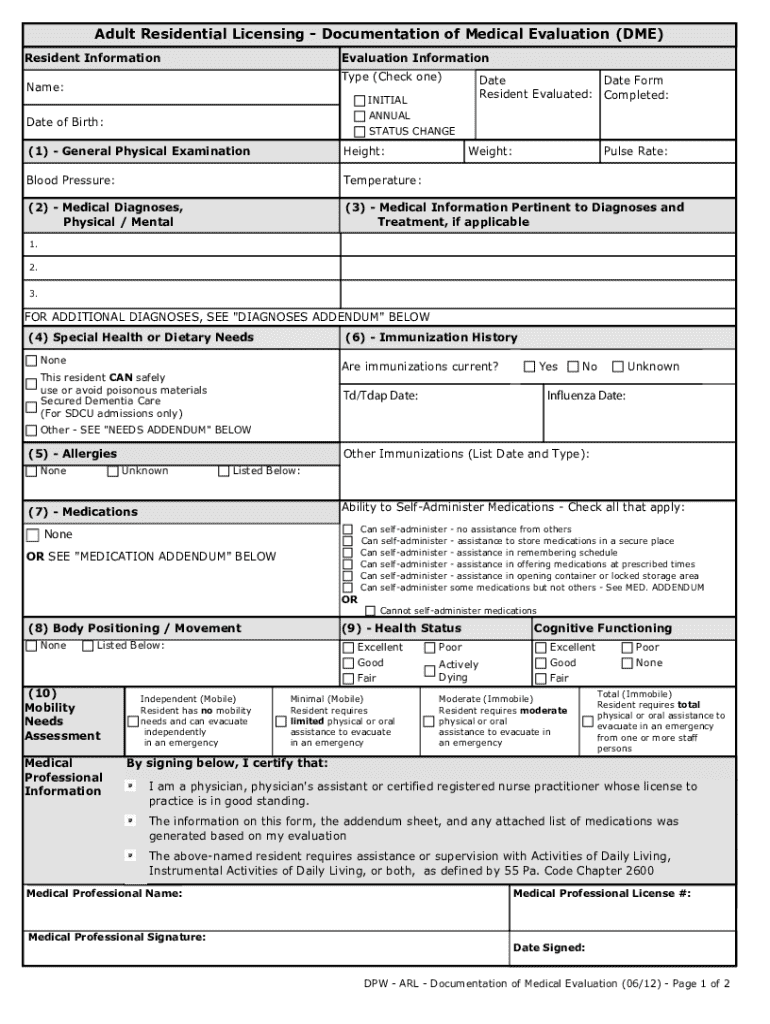
The "Documentation of Medical Evaluation" refers to a formal record utilized in adult residential facilities to document the health status of residents. This document is crucial for maintaining an accurate medical history and ensuring appropriate care is provided. It typically includes essential health details such as physical examinations, medical history, and any special health needs. The documentation process is vital for compliance with medical and legal standards, providing a structured approach to assessing and tracking the health conditions of individuals within care facilities.
Key Components of the Documentation
- Physical Examination: Detailed assessments conducted by qualified medical professionals covering vital signs and overall health.
- Medical History: A comprehensive review of the resident's past and present medical conditions.
- Special Health Needs: Specific requirements or treatments the resident may need due to chronic conditions or other health issues.
Key Elements of the Documentation of Medical Evaluation
Essential Sections of the Form
- Patient Identification: Information such as name, date of birth, and identification numbers.
- Evaluation Date: Date when the medical evaluation was conducted.
- Medical Professional's Details: Name, credentials, and contact information of the evaluating physician.
- Conclusion and Recommendations: Final assessment and suggested care plans or adjustments based on the evaluation.
Importance of Thoroughness
Ensuring the form is filled out accurately and completely is critical. This documentation serves as an official record that can influence treatment plans and facility operations. Missing or incorrect information can lead to inadequate care or legal issues for the facility.
How to Use the Documentation of Medical Evaluation
Guidance for Users
- Preparation: Gather necessary information about the resident's medical history and recent health events.
- Filling Out the Form:
- Start by accurately completing personal identification details.
- Conduct a thorough physical examination, recording all findings in the respective sections.
- Document all relevant medical history, ensuring no critical details are omitted.
- Include notes on any special health needs or current treatment plans.
Verification Process
After completion, the form should be reviewed by the medical professional to verify all data is correct. This review helps prevent potential errors or omissions.
Steps to Complete the Documentation of Medical Evaluation
- Initial Assessment: Gather comprehensive medical information about the resident.
- Conduct Physical Examination: Perform a full physical examination and note the findings.
- Document Medical History: Record previous medical conditions, surgeries, and ongoing treatments.
- Evaluate Special Health Needs: Identify and document any specific health care needs or accommodations.
- Finalize and Review: Ensure accuracy and completeness before the medical professional signs off on the document.
Practical Example
Consider a resident with a known heart condition; the form will note their current status, past treatments, and any new symptoms or changes in medication, ensuring that all involved care providers are informed and prepared to deliver appropriate care.
Who Typically Uses the Documentation of Medical Evaluation

Primary Users
- Healthcare Providers: Doctors, nurses, and other medical professionals conducting evaluations.
- Facility Administrators: Staff responsible for maintaining comprehensive records of residents' health.
- Regulatory Bodies: Authorities reviewing compliance with health regulations.
Resident and Family Involvement
In some cases, family members may be involved in supplying information for the medical history section or understanding the care plan recommendations.
Legal Use of the Documentation of Medical Evaluation
Compliance and Regulations
- HIPAA Compliance: Ensures resident information is protected and shared according to privacy laws.
- State Regulations: Varies by state but generally requires thorough documentation and regular updates to resident health evaluations.
- Facility Requirements: Each facility may have its own guidelines that align with state and federal laws for document completion and handling.
State-Specific Rules for the Documentation of Medical Evaluation
Variations Across States
While the core form content remains largely similar, specific requirements can differ, such as:
- Frequency of Evaluation: Some states require annual updates, while others may have biannual requirements.
- Specific Data Points: Certain states may require additional information, such as mental health evaluations or specific chronic illness monitoring data.
Implementation Examples
In California, for example, evaluations might require additional mental health assessments, reflecting the state's emphasis on comprehensive resident care.
Important Terms Related to Documentation of Medical Evaluation
Glossary of Key Terms
- DME (Documentation of Medical Evaluation): The shorthand commonly used for this form.
- ESIGN Act: The Electronic Signatures in Global and National Commerce Act, which ensures electronic signatures are legally recognized.
- OAuth 2.0: An authentication protocol used to secure access to sensitive information.
Providing a clear understanding of these terms helps ensure that all parties involved are familiar with the regulations and terminology critical to compliant documentation practices.