Key Elements of the Medical History Form
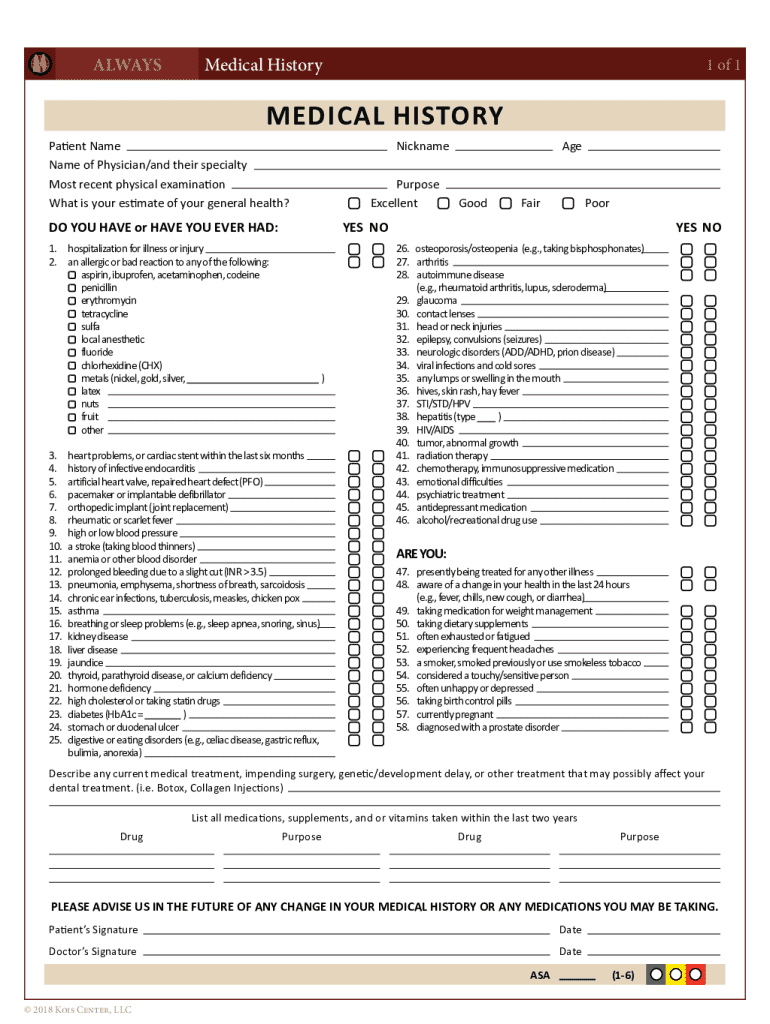
The Medical History form is designed to capture comprehensive health information from a patient, forming the backbone of medical assessments. Critical elements include:
- Personal Information: Basic details such as full name, date of birth, and contact information are required to identify the patient.
- Past Illnesses and Surgeries: Patients must list any previous medical conditions and surgeries, as this history can significantly influence current and future medical treatments.
- Allergies: Information about allergies, particularly to medications, is crucial. This prevents adverse reactions and guides prescription choices.
- Medications and Supplements: Current prescriptions and over-the-counter medications, including supplements, are documented to avoid drug interactions.
- Family Medical History: Recording any hereditary conditions in immediate family members helps assess risk factors for certain diseases.
Each of these elements is meticulously designed to provide healthcare providers a nuanced understanding of the patient's health.
Steps to Complete the Medical History Form
Completing a Medical History form requires careful attention to detail. Follow these steps for accurate submission:
- Collect Necessary Information: Gather recent medical reports, a list of current medications, and any allergy information.
- Start with Personal Details: Enter your full name, age, and contact information. Ensure details are current to maintain effective communication.
- Document Medical Conditions: List past and present medical conditions, including chronic diseases. Provide dates and relevant details to enhance accuracy.
- Note Allergies and Reactions: Highlight any known allergies to drugs, foods, or environmental factors, along with the type of reaction experienced.
- List Current Medications: Include prescription drugs, over-the-counter medicines, and any supplements.
- Review Family History: Specify any prevalent medical conditions in immediate family members to predict potential hereditary issues.
- Finalize and Review: Double-check all entries for accuracy, ensuring no critical information is omitted.
Legal Use of the Medical History Form
Medical History forms are integral to healthcare settings and are subject to strict legal standards to protect patient information. Key legal considerations include:
- Confidentiality: Under HIPAA regulations, medical history information must be handled with utmost confidentiality to protect patient privacy.
- Informed Consent: Patients provide consent for their medical history to be used for diagnosis, treatment, and insurance purposes.
- Data Security: Practices must ensure data is securely stored, often using encrypted electronic medical record systems.
- Legal Compliance: Failure to comply with regulations can lead to legal penalties and jeopardize patient trust.
These legal frameworks ensure the secure and ethical use of medical history information.
Who Typically Uses the Medical History Form
Medical History forms are widely used by various healthcare professionals and institutions. The primary users include:
- Doctors and Specialists: Physicians use the form for clinical assessments, treatment planning, and patient management.
- Dentists: Dental professionals reference medical history during evaluations to identify risks related to oral health procedures.
- Hospitals and Clinics: Institutions utilize these forms during patient intake for both emergency and routine visits.
- Allied Health Professionals: Physiotherapists and dietitians use medical history data to tailor treatments and dietary plans.
Each user group relies on comprehensive and accurate health histories to deliver effective care.

Importance of a Medical History Form
The importance of a medical history form cannot be overstated. It serves several critical functions:
- Diagnosis and Treatment: Provides a health overview that aids accurate diagnosis and effective treatment planning.
- Risk Assessment: Identifies potential health risks and contraindications, driving informed medical decisions.
- Continuity of Care: Enables seamless communication across different healthcare providers, ensuring continuity and comprehension in patient care.
- Preventive Measures: Helps in identifying lifestyle adjustments and preventive measures for diseases with hereditary predispositions.
Through these functions, the form becomes a cornerstone in patient-centered healthcare.
Examples of Using the Medical History Form
Real-world applications of a Medical History form demonstrate its utility in varied scenarios:
- Pre-Surgical Evaluation: Surgeons assess medical history to plan anesthesia and manage any pre-existing conditions.
- Emergency Care: Quick access to a patient's medical history ensures immediate and accurate treatment during emergencies.
- Chronic Disease Management: Forms are regularly updated to track progress and adapt chronic disease management strategies.
- New Patient Visits: Physicians use the form during initial consultancy to establish a baseline for all future care plans.
Each example underscores the form’s role in enhancing medical care quality and patient safety.
Digital vs. Paper Versions of the Medical History Form
While both digital and paper versions are commonly used, key differences affect their deployment in healthcare systems:
- Ease of Use: Digital forms are easily updated and stored, offering quick access and reducing paper clutter.
- Integration with EMR: Digital forms integrate seamlessly with electronic medical records (EMR), allowing for real-time data sharing.
- Accessibility: Digital access is pivotal for telehealth services, remote patient monitoring, and healthcare app integrations.
- Security Concerns: Digital records require robust cybersecurity measures to safeguard against unauthorized access.
Both formats have their benefits, but digital versions significantly enhance functionality and efficiency in modern healthcare settings.
Software Compatibility and Medical History Forms
Medical History forms benefit from compatibility with various healthcare software, streamlining administration and care coordination:
- Electronic Health Record (EHR) Systems: Integration ensures consistent data entry and easy retrieval across different healthcare platforms.
- Practice Management Software: These solutions automate patient record management, scheduling, and billing, utilizing medical history data.
- Cloud-Based Solutions: Platforms like DocuHub enable secure form editing, sharing, and archiving, enhancing collaboration among healthcare providers.
These software tools optimize workflows, ensure accurate record-keeping, and facilitate better healthcare outcomes.