01. Edit your cms 1500 insurance claim form online
Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send form cms 1500 free via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out claim form cms1500 with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
Click ‘Get Form’ to open the CMS-1500 claim form in the editor.
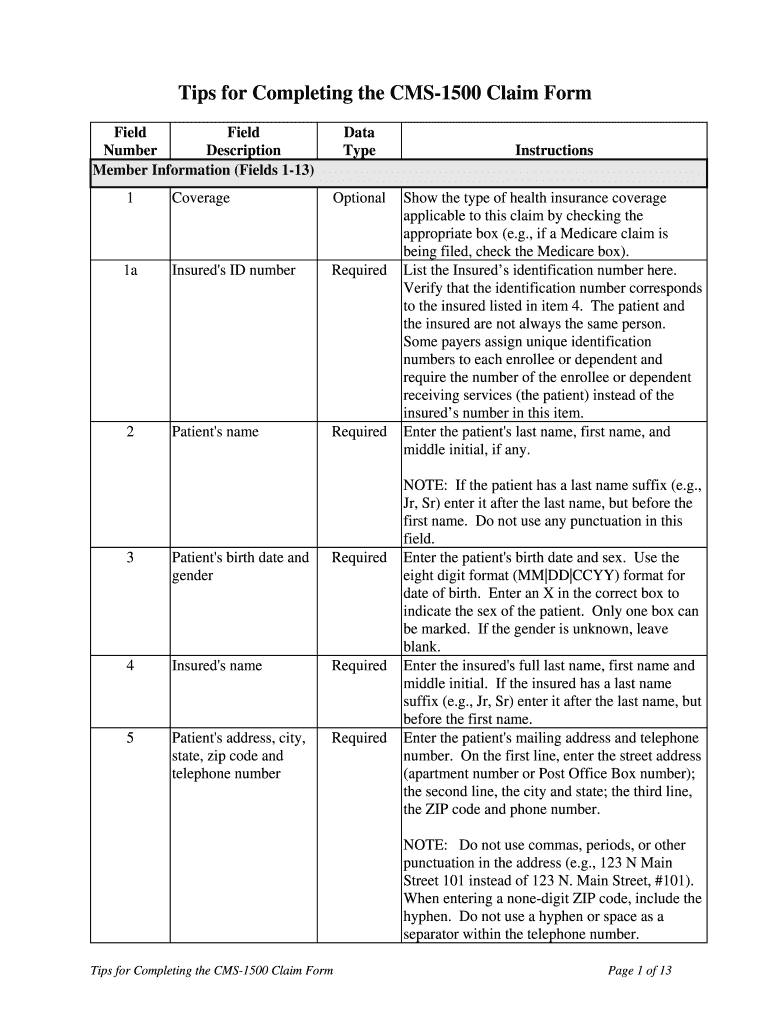
Begin by filling out the Member Information section (Fields 1-13). Indicate the type of health insurance coverage applicable to this claim by checking the appropriate box. Enter the insured's ID number, patient's name, birth date, and gender accurately.
Continue with Fields 6-9, detailing the patient's relationship to the insured and any other insurance information if applicable. Ensure that all addresses are entered without punctuation.
In Fields 10a-c, indicate if the patient’s condition is related to employment or accidents. Complete Field 11 with the insured’s policy group number.
Proceed to Provider of Service or Supplier Information (Fields 14-33). Fill in dates of service, procedure codes, and charges accurately. Ensure that you enter your NPI and tax ID correctly.
Start using our platform today for free to streamline your CMS-1500 claims process!
CMS-1500 form pdfUB-04 claim formPrintable CMS-1500 formFree CMS-1500 formCMS 1500 form boxesWhere can i get a CMS 1500 formHow do i get a CMS 1500 formCompleted CMS-1500 form Sample pdf
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
by JB Doe The revised 1500 Claim Form expands the length of some existing fields, incorporates several new fields, and accommodates use of your taxonomy. Some importantRead more
The CMS-1500 form is the standard paper claim form used to bill Medicare and many other payers for services provided by physicians and other healthcareRead more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.