Health claim form 1500 pdfHealth claim form 1500 printableCMS 1500 form pdfHealth claim form 1500 templateHealth claim form 1500 pdf downloadPrintable CMS 1500 formCMS 1500 form downloadHealth insurance claim FORM 1500 fillable PDF free
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
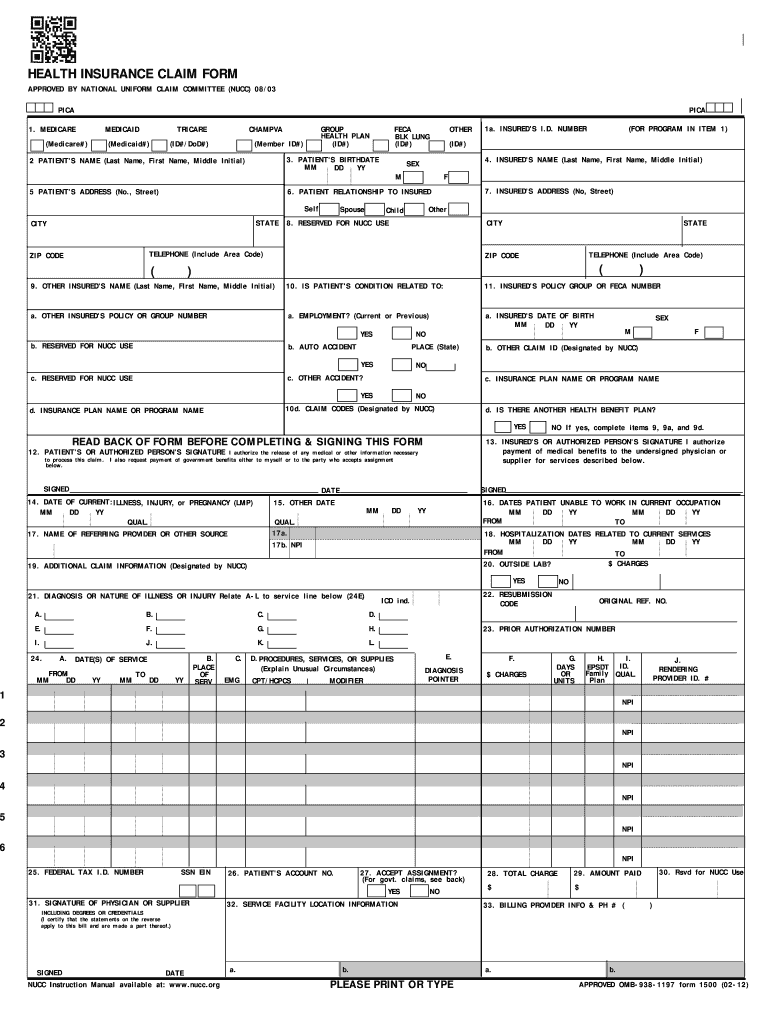
The CMS-1500 form is the standard paper claim form used to bill Medicare and many other payers for services provided by physicians and other healthcareRead more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.