Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send it via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out withdrawal claim form with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
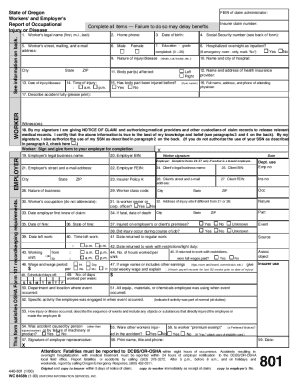
Click ‘Get Form’ to open the withdrawal claim form in the editor.
Begin by entering the court address and case number at the top of the form. This information is crucial for identifying your claim within the court system.
Indicate whether you are filing on behalf of a deceased individual or a protected person by checking the appropriate box.
Fill in your name and contact details, including phone number, fax number, email, and attorney registration number if applicable. This ensures that all communications regarding your claim can be directed to you.
In the section describing the nature of your claim, provide a clear and concise explanation of what your claim entails. This helps clarify your position regarding the estate.
Choose whether you wish to withdraw your claim or acknowledge that it has been satisfied by checking the corresponding box.
Finally, sign and date the form. Below your signature, type or print your name, address, and telephone number for verification purposes.
Start using our platform today to fill out your withdrawal claim form easily and for free!
Withdrawal claim form pdfNotice of Withdrawal of Claim formWithdrawal claim form onlineAlexander FORBES claim forms pdfFree withdrawal claim formAlexander Forbes withdrawal FormsAlexander Forbes provident fund withdrawal processAlexander Forbes withdrawal online
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
Withdrawal of Claim | Central District of California
Select Bankruptcy menu. Select Claim Actions. Enter the case number using correct format and ensure case name and number match the document you are filing.Read more
MAIL CLAIM FORM TO: Health Care Account Service Center. Claim Submission / Withdrawal Request Form: PO Box 981506. El Paso, TX 79998-1506. Fax: 915-231-1709.
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.