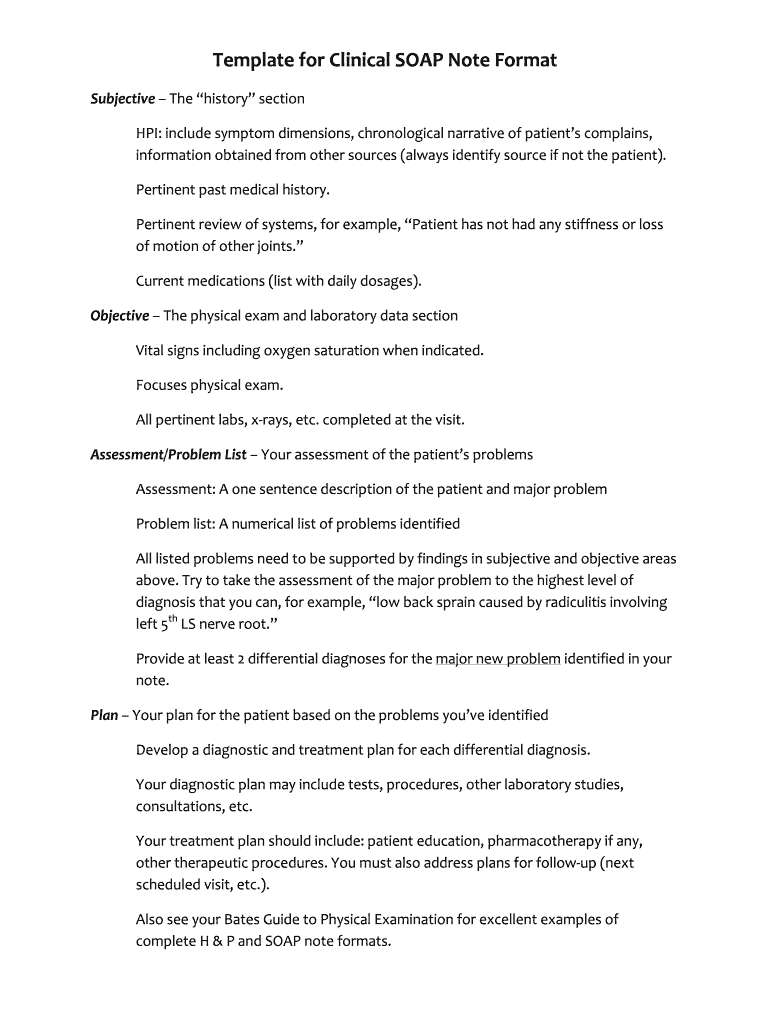
Definition and Meaning of SOAP Narrative
A SOAP narrative is a structured method of documentation used primarily in healthcare and emergency services to create a detailed account of a patient’s condition and treatment. The acronym SOAP stands for Subjective, Objective, Assessment, and Plan. Each section serves a distinct purpose in capturing the patient's story and guiding the healthcare provider's actions.
Subjective
- The subjective portion includes the patient’s personal experience of their symptoms. This often features quotes from the patient and covers their medical history and the current issues they are facing.
- Example: A patient might express, "I have had a headache for three days, and it feels like a pounding sensation on one side of my head."
Objective
- This section encompasses measurable data collected during the examination, such as vital signs, physical findings, and lab results. Objective data adds an evidence-based component to the narrative.
- Example: Documenting a patient’s blood pressure as 140/90 mmHg and noting a fever of 101°F.
Assessment
- The assessment includes the clinician’s evaluation, forming a diagnosis or a problem list based on the subjective and objective findings. This section blends clinical reasoning with the patient’s history.
- Example: "The patient presents with symptoms consistent with migraine headache, considering the recent history of stress and poor sleep."
Plan
- The plan outlines the next steps in treatment and management, providing the framework for follow-up and evaluation. This can include medications, referrals, and lifestyle modifications.
- Example: "Prescribe ibuprofen 400 mg every six hours as needed for pain, and schedule a follow-up appointment in a week to reassess."
Key Elements of SOAP Narrative
A comprehensive SOAP narrative consists of various key elements that ensure clarity, consistency, and adherence to documentation standards. These include:
- Clarity and Conciseness: Each section should be direct and succinct, enabling quick understanding by other healthcare providers.
- Chronological Order: Events or treatments should be documented in order of occurrence to maintain a clear timeline.
- Patient Focus: Each entry should center around the patient's perspective, highlighting their experiences and feedback.
Who Typically Uses SOAP Narratives
SOAP narratives are commonly utilized by various healthcare professionals, including but not limited to:
- Physicians and Nurses: For documenting patient visits, assessments, and treatment plans.
- Emergency Medical Technicians (EMTs): To create patient care reports (PCR) detailing pre-hospital care.
- Mental Health Professionals: To track patient progress and therapy notes effectively.
- Physical Therapists: To outline treatment goals and patient feedback on progress.
Examples of Using SOAP Narrative in Practice
Real-world examples of SOAP narratives can range from hospital settings to outpatient clinics. These narratives help maintain clear communication among teams.
-
Emergency Services: An EMT might document:
- Subjective: "The patient reports chest pain radiating to the left arm."
- Objective: "Pulses are strong; the patient has an elevated heart rate of 110 bpm."
- Assessment: "Possible acute myocardial infarction."
- Plan: "Administer aspirin and transport to the nearest emergency room."
-
In Clinical Settings: A nurse’s SOAP note during a routine check-up could read:
- Subjective: "Patient states, 'I've been feeling very tired lately.'"
- Objective: "Lab results indicate anemia with hemoglobin at 10 g/dL."
- Assessment: "Fatigue secondary to diagnosed anemia."
- Plan: "Discuss iron supplementation and dietary modifications."
Steps to Complete a SOAP Narrative
Creating an effective SOAP narrative involves a systematic approach:
- Gather Information: Collect comprehensive patient data through interviews and examinations.
- Document Subjective Findings: Write down the patient’s own words regarding their symptoms and concerns.
- Record Objective Findings: Include measurable outcomes such as vital signs and relevant lab results.
- Assess the Information: Combine subjective and objective inputs to form a coherent assessment.
- Create a Plan: Outline specific actions for treatment, follow-up, and further assessments.
Legal Use of SOAP Narrative
SOAP narratives are not only essential for clinical practice but also hold legal significance. They serve as a legal document that can provide evidence of care provided, informed consent, and adherence to medical standards. Proper documentation protects both the healthcare provider and patient by ensuring clear communication and accountability.
- Compliance with Regulations: SOAP narratives should meet the legal standards set by health regulations.
- Record Keeping: Accurate documentation supports healthcare audits and investigations into patient care quality.
Important Terms Related to SOAP Narrative
Understanding specific terminology associated with SOAP narratives enhances clarity and precision. Some relevant terms include:
- Patient Care Report (PCR): A formal document outlining the care provided to a patient by EMS personnel.
- Clinical Audit: A systematic review of clinical practices to ensure quality and adherence to guidelines.
- Differential Diagnosis: The process of distinguishing between two or more conditions that share similar signs or symptoms.
By effectively employing the SOAP narrative format, healthcare professionals can ensure comprehensive, organized, and clear documentation that enhances patient care.