Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send it via email, link, or fax. You can also download it, export it or print it out.
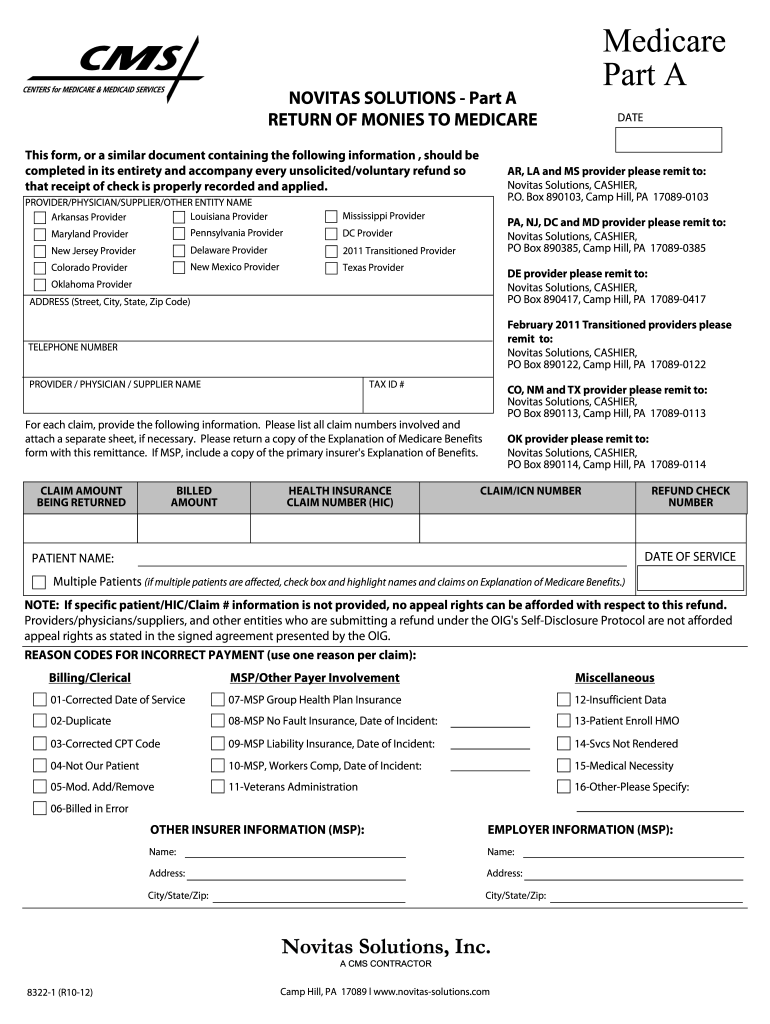
How to use or fill out Medicare form 8322 1a with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
Click ‘Get Form’ to open the Medicare form 8322 1a in the editor.
Begin by filling in your name as the provider, physician, or supplier at the top of the form. Ensure you include your complete address and telephone number for accurate processing.
In the claims section, list all claim numbers involved in the refund. If necessary, attach a separate sheet for additional claims. Remember to include a copy of the Explanation of Medicare Benefits.
Indicate the claim amount being returned and provide details such as billed amount, health insurance claim number (HIC), and date of service.
If multiple patients are affected, check the box provided and highlight their names on the Explanation of Medicare Benefits.
Select appropriate reason codes for incorrect payment from the provided list, ensuring you use one reason per claim.
Complete any additional sections regarding other insurer information and employer information if applicable.
Start using our platform today to fill out your Medicare form 8322 1a easily and for free!
We've got more versions of the medicare form 8322 1a form. Select the right medicare form 8322 1a version from the list and start editing it straight away!
Medicare form 8322 1a pdfMedicare form 8322 1a pdf downloadMedicare form 8322 1a downloadMedicare form 8322 1a onlineMedicare form 8322 1a instructionsHow to fill out medicare form 8322 1aNgs Medicare voluntary refund FormMedicare recoupment form
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
MSU Retiree Open Enrollment Benefits Guide for the 2026
Retiree Open Enrollment/Change Form. Coverage Effective 1/1/2026. Complete this form to enroll in, change, or cancel health, dental, or life insuranceRead more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.