


Definition and Meaning of interRAI Acute Care Assessment Form
The interRAI Acute Care Assessment Form is a standardized tool developed for the comprehensive evaluation of patients in acute care settings. It aims to gather detailed information regarding a patient's health conditions, social circumstances, and functional abilities to inform treatment decisions and care planning. The form includes various sections covering key aspects such as basic identification information, medical history, cognitive function, emotional wellbeing, and physical health metrics.
The underlying philosophy of the interRAI tool is to provide a person-centered approach to healthcare. This means that care assessments should not only focus on clinical data but also on patients' preferences and life circumstances, considering factors that affect their overall wellness. As a result, the interRAI Acute Care Assessment Form supports health professionals in delivering tailored interventions that enhance patient outcomes during their care journey.
The form serves multiple objectives:
- Facilitating a holistic understanding of patient needs
- Supporting data collection for compliance with healthcare regulations
- Enabling continuity of care during transitions between healthcare settings
Key Elements of the interRAI Acute Care Assessment Form
The interRAI Acute Care Assessment Form is organized into several critical sections that capture comprehensive patient data:
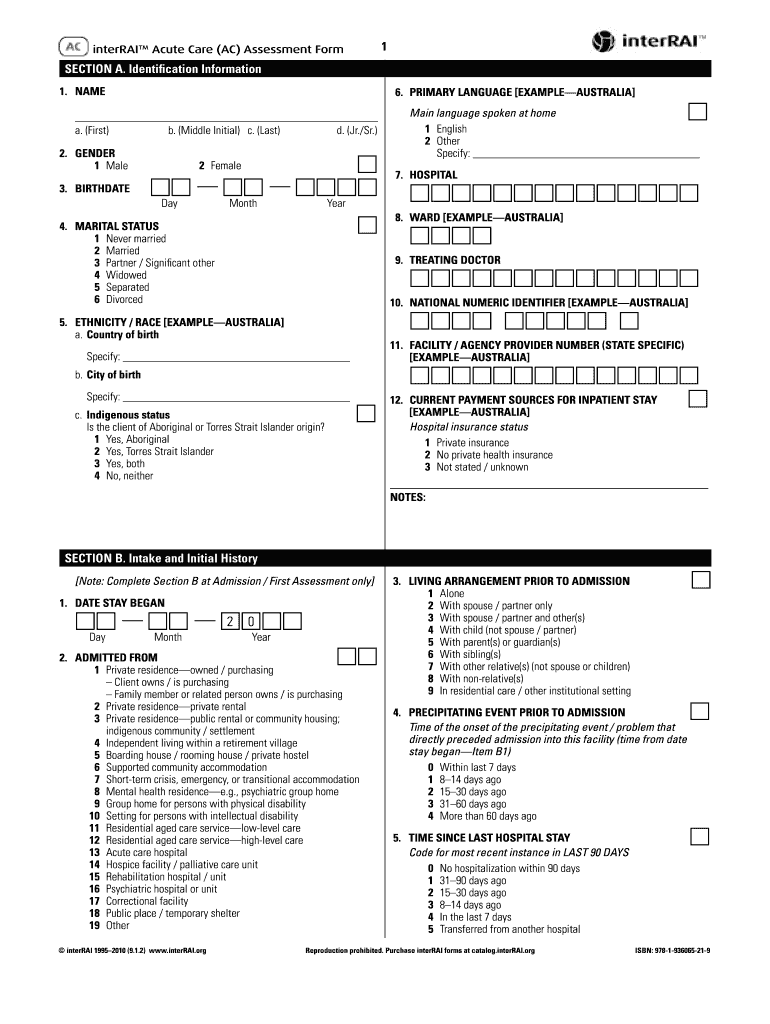
- Identification Section: Records basic information such as name, date of birth, and emergency contact details.
- Intake History: Includes past medical and surgical history, as well as a review of medications and allergies.
- Cognitive and Functional Assessments: Evaluates cognitive functioning, memory problems, and the individual's ability to perform activities of daily living.
- Communication Abilities: Documents the patient's ability to communicate effectively, including any barriers to communication.
- Mood and Behavior Evaluations: Assesses emotional health and any behavioral concerns that may impact treatment.
- Nutritional Status: Reviews dietary habits, weight changes, and overall nutrition.
- Skin Condition: Examines skin integrity and identifies any risk factors for pressure ulcers.
- Medications and Treatments: Details current medications, their purpose, and any necessary adjustments during illness.
- Discharge Planning: Identifies discharge needs and necessary follow-up care, allowing for a smooth transition from hospital to home or another care facility.
The integration of these sections ensures that healthcare providers have a comprehensive view of the patient's status, facilitating well-informed care planning and coordination among multidisciplinary teams.
Steps to Complete the interRAI Acute Care Assessment Form
Completing the interRAI Acute Care Assessment Form involves a systematic approach to ensure all relevant patient data is accurately captured. Here are the essential steps:
- Gather Patient Information: Begin by collecting basic patient demographic data, including name, date of birth, and other identifiers.
- Review Medical History:
- Document any prior health conditions and significant medical history.
- List current medications and any known allergies.
- Conduct Assessments:
- Use standardized tools for cognitive and functional assessment to determine patient capabilities and needs.
- Evaluate communication abilities, capturing any barriers or challenges.
- Assess Nutrition and Skin Condition:
- Measure dietary habits and assess any nutritional deficiencies.
- Examine the patient's skin for any issues, especially if there are concerns about immobility.
- Evaluate Mood and Behavior:
- Use observational assessments and structured interviews to gauge emotional wellbeing and any behavioral issues.
- Finalize Discharge Planning:
- Discuss the results with the patient and their family to outline follow-up needs and plan for discharge.
- Document all findings comprehensively to create an actionable care plan.
Completing each section carefully enhances the utility of the form, promoting effective communication among medical teams and improving patient care overall.
Legal Use of the interRAI Acute Care Assessment Form
The interRAI Acute Care Assessment Form is legally recognized for use in patient assessments across various healthcare settings. Its design adheres to best practices aimed at ensuring patient safety, quality of care, and regulatory compliance. Compliance with federal and state laws regarding patient information is paramount when utilizing this assessment form.
Healthcare facilities are required to follow specific legal guidelines concerning data privacy and patient rights when completing and storing assessment forms. These legal requirements may include:
- HIPAA Compliance: Adherence to the Health Insurance Portability and Accountability Act regulations to protect patient health information.
- Data Retention Policies: Establishing protocols for how long patient assessments must be retained as part of medical records.
- Audit Trails: Maintaining records that document the completion and modification history of patient assessments to ensure transparency and accountability.
The legal use of the interRAI Acute Care Assessment Form also extends to electronic versions that may be part of larger health information systems, which must meet stringent security requirements to safeguard patient data.
Important Terms Related to the interRAI Acute Care Assessment Form
Understanding specific terminology used in relation to the interRAI Acute Care Assessment Form is critical for healthcare professionals. Key terms include:
- Assessment Domains: Categories within the form aimed at evaluating specific areas of patient health that influence care strategies.
- Person-Centered Care: A care approach that involves the patient in decisions about their treatment, ensuring that their preferences are respected.
- Multidisciplinary Team: A collaborative group of healthcare professionals from various specialties working together to provide comprehensive care.
- Admission Criteria: Guidelines that determine whether a patient qualifies for acute care services based on their health assessment results.
- Clinical Indicators: Measurable factors that signal the patient's health status or changes in their condition, useful for guiding treatment decisions.
This foundational knowledge aids healthcare providers in effectively communicating with colleagues, ensuring a shared understanding of patient needs, and implementing appropriate care interventions.
Examples of Using the interRAI Acute Care Assessment Form
Utilizing the interRAI Acute Care Assessment Form involves practical applications across various clinical scenarios. Consider the following example cases:
- Post-Surgery Evaluation: In an acute care setting, a patient who recently underwent major surgery may be assessed using the form to monitor recovery. The nurse would complete sections evaluating pain levels, mobility, and emotional state to create an appropriate post-operative care plan.
- Emergency Room Admit: A patient presenting with an acute condition, such as chest pain, would have their acute care needs assessed immediately. The information collected via the form enables rapid identification of critical health issues to address upon admission.
- Interdisciplinary Review: Following assessment, an interdisciplinary team meeting might occur where the data collected from the interRAI form are reviewed to create a coordinated treatment plan based on collective expertise.
These examples illustrate the form's utility in facilitating comprehensive patient evaluations, timely interventions, and collaborative care planning among healthcare professionals.