Definition & Meaning
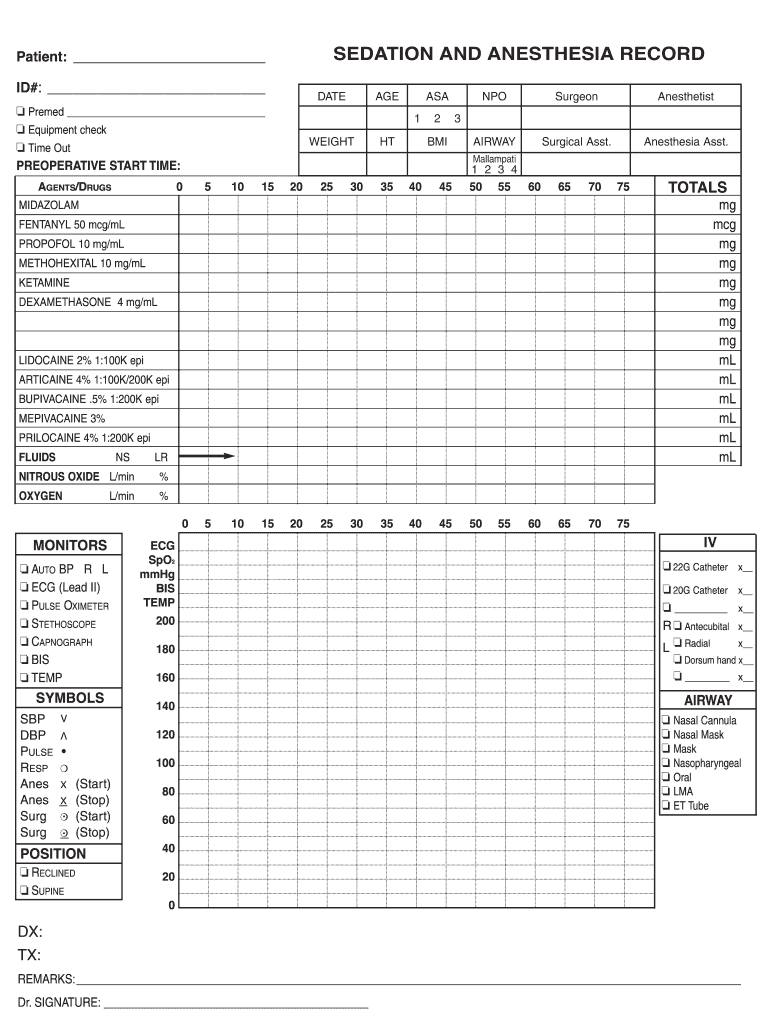
The sedation anesthesia record template is a structured document used in medical settings to document the administration of sedation and anesthesia during procedures. This record is crucial for ensuring patient safety and improving the quality of care. It typically includes sections for patient identification, drug administration details, monitoring parameters, and post-procedure recovery notes. By providing a standardized format for recording anesthesia information, the template helps clinicians maintain accurate records, which is vital for legal compliance and continuity of care.
Key Components of the Template
- Patient Identification: Basic information such as name, age, medical history, and procedure details is documented to provide context for the anesthesia administered.
- Drug Administration: This section outlines the specific sedatives or anesthetics used, their dosages, and the timing of administration, ensuring precise records of what was given to the patient.
- Monitoring Data: Continuous monitoring is vital during sedation. The template includes areas to document vital signs, level of sedation, and any adverse reactions observed during the procedure.
- Post-Procedure Notes: Follow-up information detailing the patient’s recovery, discharge criteria, and any complications can be recorded, which assists in evaluations of the procedure's effectiveness.
Key Elements of the Sedation Anesthesia Record Template
A comprehensive sedation anesthesia record template contains several key elements that ensure complete documentation of the sedation process, enhancing both patient safety and clinical accountability.
Essential Sections of the Template
- Preoperative Assessment: This includes evaluations made before the administration of anesthesia, such as relevant medical history and current medications.
- Intraoperative Monitoring: This section captures vital signs (heart rate, blood pressure, oxygen saturation) and level of sedation during the procedure. It helps ensure patient stability and safety.
- Drugs and Dosages: All anesthetics and sedatives used during the procedure should be logged, including specific dosages, administration routes, and times of administration.
- Recovery Evaluation: Post-anesthesia, the patient should be assessed regarding their responsiveness, airway management, and any side effects experienced.
Including these components can enhance the quality of care provided by ensuring that all necessary information is captured and can be reviewed if needed.
Steps to Complete the Sedation Anesthesia Record Template
Properly completing the sedation anesthesia record template is crucial for legal compliance and patient safety. Here is a step-by-step guide on how to accurately fill out this essential document.
-
Gather Patient Information: Start by entering the patient's name, age, medical record number, and the procedure being performed.
-
Document Preoperative Assessment: Include any pre-existing conditions, allergies, and the consent process. This information ensures that the medical team is aware of the patient’s health status before administering anesthesia.
-
Record Drug Administration: As sedatives or anesthetics are administered, meticulously log the name of the drug, dosage, route of administration, and the time administered. Ensure all entries are accurate and legible.
-
Monitor and Record Vital Signs: Continuously monitor vital signs during the procedure and note these in the appropriate sections. This should include heart rate, blood pressure, respiratory rate, and oxygen saturation levels.
-
Post-Procedure Evaluation: After the procedure, evaluate the patient’s recovery and document any complications or side effects experienced, as well as discharge criteria.
-
Review for Completeness: Before finalizing the record, review it to ensure that all sections are filled out clearly and completely, minimizing the risk of discrepancies in patient care.
Each step is critical to ensuring comprehensive and accurate documentation that can be referenced for future medical decisions.
Who Typically Uses the Sedation Anesthesia Record Template
The sedation anesthesia record template is widely utilized by various healthcare professionals involved in sedation and anesthetic procedures. Understanding who uses this template can enhance its effectiveness and compliance within clinical settings.
Principal Users of the Template
- Anesthesiologists: Often the primary users, anesthesiologists administer anesthesia and document the entire process for safety and legal compliance.
- Nurses: Operating room and recovery room nurses rely on the template to monitor and document patient vitals and recovery progress, collaborating closely with anesthesiologists.
- Surgeons: Surgeons need access to sedation records to understand the anesthesia state of their patient during surgical interventions, ensuring a smooth workflow and patient safety.
- Dental Professionals: In dental practices, oral surgeons and dental anesthesiologists use this template to document sedation protocols during procedures requiring anesthesia.
By encompassing the roles of these healthcare providers, the template facilitates a cooperative approach to patient care during procedures requiring sedation.
Legal Use of the Sedation Anesthesia Record Template
Legal compliance is a significant aspect of using the sedation anesthesia record template. Proper documentation not only ensures adherence to healthcare regulations but also protects both healthcare providers and patients.
Legal Considerations
- Medical Record Keeping Standards: The template should align with the standards set forth by state and federal regulations concerning medical documentation. This includes ensuring that records are complete, timely, and accurate.
- Informed Consent: Documenting informed consent is crucial prior to anesthesia administration. This protects providers legally and ensures patients are aware of risks associated with sedation.
- Audits and Legal Defense: A well-maintained sedation anesthesia record can serve as a valuable defense tool in case of legal inquiries or malpractice claims. It provides an official account of the care provided, which can be critical in resolving disputes.
- Retention Policies: Healthcare facilities are subject to specific laws that mandate how long medical records must be retained. The completion of the anesthesia record should adhere to these policies for legal compliance.
Recognizing these legal implications enhances the conscientious use of the sedation anesthesia record template in clinical practice.