


Understanding the Letter of Medical Necessity for HSA
The Letter of Medical Necessity (LMN), particularly for Health Savings Accounts (HSAs), is critical for patients seeking reimbursement for expenses not typically covered by standard health insurance policies. The LMN acts as a formal statement from a licensed healthcare provider, attesting that a particular medical treatment or service is essential for the patient’s health.
Key Features of the Letter of Medical Necessity
- Purpose: The LMN is utilized to justify claims for medical expenses under an HSA. It verifies to the account administrators or insurers that the service or treatment is necessary for the patient's health.
- Provider Certification: A licensed healthcare provider must sign the letter, reinforcing the legitimacy of the medical claim.
- Detailed Information: The document must include specific patient details, diagnosis, treatment plan, and expected outcome to assist in the claims process effectively.
Components of an Effective Letter of Medical Necessity
An effective LMN carries essential information that aligns with IRS guidelines for reimbursement. Key components include:
- Patient Information: Full name, date of birth, and HSA account number if applicable.
- Diagnosis: Detailed assertion of the patient’s medical condition or diagnosis linked to the recommended treatment.
- Treatment Description: Explanation of the specific health service or item necessary for treatment, including medical equipment or therapy.
- Rationale: Justification of why the treatment is deemed medically necessary, including expected health benefits and improvements.
- Provider Contact: The healthcare provider’s contact information and signature for authentication.
Sample Letter of Medical Necessity for HSA
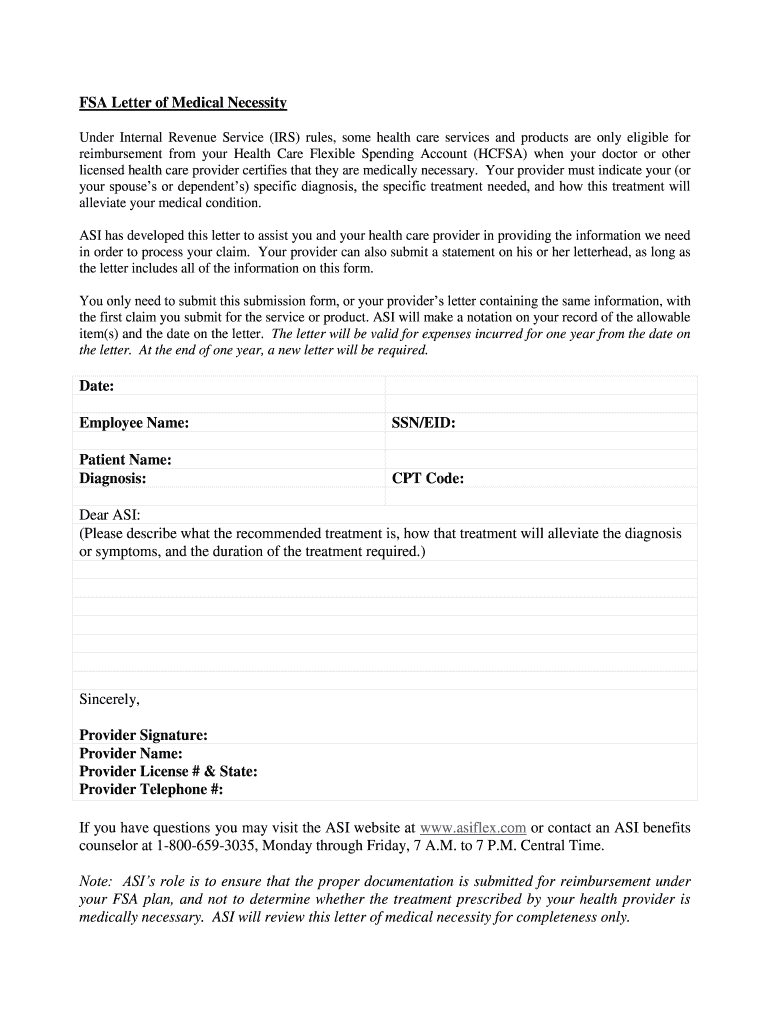
Below is a basic structured example of a letter that can guide healthcare providers in drafting an LMN for HSA reimbursements:
[Healthcare Provider’s Letterhead] [Date]
[Patient's Name] [Patient's Address] [City, State, Zip Code]
Subject: Letter of Medical Necessity for [specific treatment/service]
To Whom It May Concern:
I, [Provider’s Name], am a licensed [Provider’s Title, e.g., physician, therapist], and am currently treating [Patient's Name] for [Diagnosis].
The purpose of this letter is to confirm that [specific service or item], provided by [Provider or service provider’s name], is medically necessary for [Patient's Name]. The treatment is required to address [explain the condition] and is expected to result in [explain expected benefits].
Please find my contact details below for any further verification required.
Sincerely,
[Provider’s Signature]
[Provider’s Name]
[Provider’s Contact Information]
Compliance with IRS Guidelines
When filing for HSA reimbursements, it is imperative that the LMN complies with IRS requirements. This ensures that the reimbursement claims are processed smoothly without any issues. The Internal Revenue Service outlines that the expense must be primarily for medical care to be tax-deductible, thus necessitating the LMN.
Situations Requiring a Letter of Medical Necessity
The LMN may be necessary for various treatments or services, such as:
- Durable Medical Equipment (DME): Items like wheelchairs or oxygen equipment.
- Home Health Aide Services: Justification for care provided at home when medically necessary.
- Therapeutic Services: Including physical, occupational, or speech therapy.
- Alternative Medicine: Services such as acupuncture or chiropractic care when recommended by a licensed practitioner.
Tips for Providers When Drafting an LMN
When creating a Letter of Medical Necessity for HSAs, healthcare providers should consider the following:
- Clarity: Use clear and precise language.
- Specificity: Tailor the letter to the individual needs and context of the patient's condition and treatment.
- Documentation: Attach any relevant medical records or additional documentation that supports the necessity of the proposed treatment.
Conclusion: Importance of the Letter of Medical Necessity
The Letter of Medical Necessity is a vital tool for patients to ensure that they can access the medical treatments they need while allowing them to utilize their Health Savings Accounts efficiently. Familiarizing both providers and patients with the proper components and requirements of this document can facilitate smoother processing of claims and reimbursement.



