Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send md india claim form part a and b pdf via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out india claim form with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
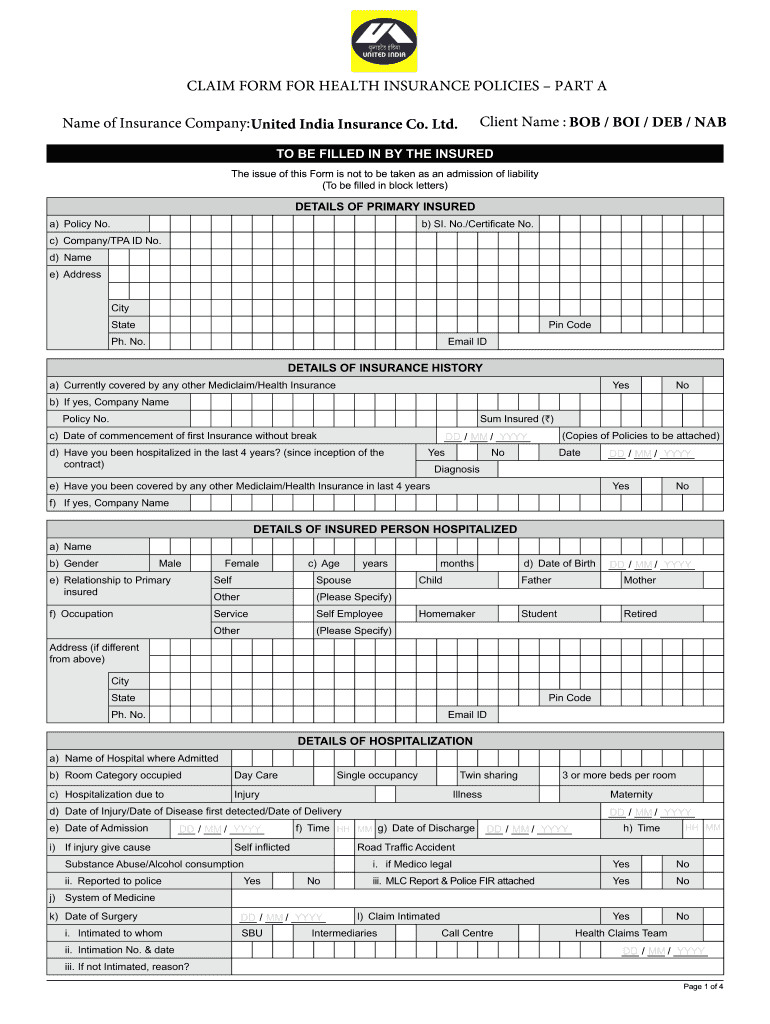
Click ‘Get Form’ to open the india claim form in the editor.
Begin by filling in your personal details in block letters, including your name, address, and contact information. Ensure accuracy as this information is crucial for processing your claim.
Provide details of your insurance history. Indicate if you are currently covered by any other health insurance and include relevant policy numbers and sum insured amounts.
Complete the section regarding the insured person hospitalized. Fill in their name, age, gender, relationship to the primary insured, and occupation.
Detail the hospitalization specifics such as hospital name, admission dates, and reasons for hospitalization. Be thorough to avoid delays.
List all treatment expenses claimed under various categories like pre-hospitalization and post-hospitalization costs. Attach necessary documents as per the checklist provided.
Finally, review all entries for accuracy before signing the declaration at the end of the form. This confirms that all information is true to your knowledge.
Start using our platform today to fill out your india claim form easily and efficiently!
Simply put, claim intimation is the process of notifying your insurance company about a possible future hospitalisation or an emergency hospitalisation emergency.
How to fill the new India Assurance Claim Form?
GUIDANCE FOR FILLING CLAIM FORM PART A (To be filled in by the insured) DATA ELEMENT. DESCRIPTION. FORMAT. SECTION A - DETAILS OF PRIMARY INSURED. SECTION B - DETAILS OF INSURANCE HISTORY. SECTION C - DETAILS OF INSURED PERSON HOSPITALIZED. SECTION D - DETAILS OF HOSPITALIZATION. ClaimForm.pdf - New India Assurance New India Assurance know-more health New India Assurance know-more health PDF
How do I fill out a reimbursement claim form?
If you are wondering how to fill reimbursement claim form, remember to provide accurate details and attach all necessary documents, such as your medical certificate, ID proof, and any other papers related to the claim. 6. Collect everything, arrange them date-wise and submit them to the insurance provider.
How to fill out a life insurance claim form?
If youre completing an individual claim form, youll need to fill out personal details about you and the insured, such as: Full name. Address. Date of birth. Social security number. Your relationship to the insured.
What is a claim form?
PF Form 19 is used for full withdrawal of provident fund after retirement, resignation, or termination from employment. PF Form 19: What is it, Benefits and How to Fill EPF Form - Bajaj Finserv Bajaj Finserv investments pf-form-19 Bajaj Finserv investments pf-form-19
md india claim form pdf download
India claim form pdfIndia claim form pdf downloadIndia claim form downloadClaim FORM - PART AIndia claim form onlineClaim FORM - PART A and bMd India Claim Form pdf DownloadHealth India Claim Form - PART A and b pdf
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
You have to fill out Form 19 for final settlement, Form 31 for partial EPF withdrawal, Form 10C for pension withdrawal, and Form 10D for the monthly pension after retirement or under specific conditions like inability to work, death of the EPF member. EPF Form 19: What Is It And How To Fill Form 19 For PF Withdrawal? ClearTax epf-form-19 ClearTax epf-form-19
How to fill insurance claim form part B?
(To be Filled in block letters) DETAILS OF HOSPITAL. DETAILS OF THE PATIENT ADMITTED. DETAILS OF AILMENT DIAGNOSED (PRIMARY) CLAIM DOCUMENTS SUBMITTED - CHECK LIST. ADDITIONAL DETAILS IN CASE OF NON NETWORK HOSPITAL (ONLY FILL IN CASE OF NON-NETWORK HOSPITAL) (PLEASE READ VERY CAREFULLY) DECLARATION BY THE HOSPITAL.
mdindia claim form
Form 8233 Attachment Nonresident Alien Employees India
I was a resident of India on the date of my arrival in the United States. I am not a United States citizen. I have not been lawfully accorded the privilegeRead more
File an initial application for benefits as soon as you become unemployed. You will need the following information when filing: A valid email account yourRead more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.