


Definition & Meaning
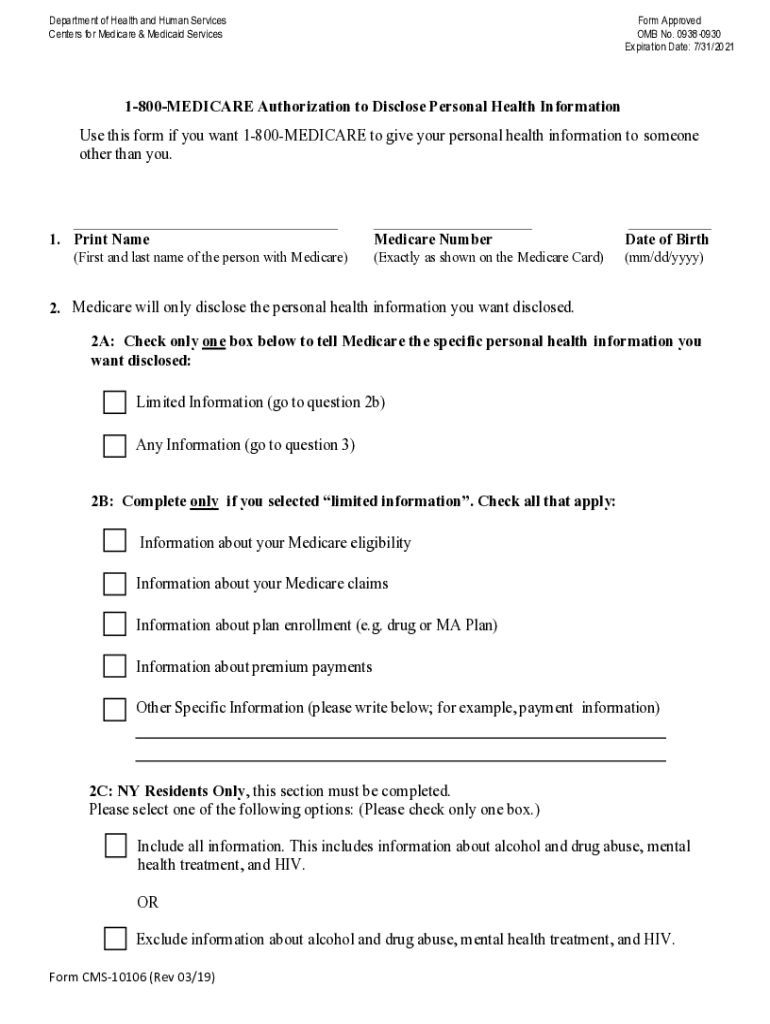
The "CMS10106 1-800-MEDICARE Authorization to Disclose Personal Health Information Form" is a vital document allowing Medicare beneficiaries to authorize the release of their personal health information to designated individuals or organizations. This authorization supports efficient communication and coordination of healthcare services, ensuring beneficiaries can access personalized care.
How to Use the CMS10106 1-800-MEDICARE Form
To use this form, beneficiaries must specify the information to be disclosed and identify the parties authorized to receive it. It's crucial for ensuring that only designated individuals have access to sensitive health information. Use cases include granting family members access to medical records or authorizing healthcare providers to share necessary details for specialized care.
How to Obtain the CMS10106 1-800-MEDICARE Form
The form is accessible via Medicare's official website or by contacting Medicare directly at their helpline, 1-800-MEDICARE. Additionally, healthcare provider offices often have copies available for their patients. Requesting through mail or visiting a local Social Security office are alternative methods.
Steps to Complete the CMS10106 1-800-MEDICARE Form
- Identify the Information: Clearly specify the type of personal health information you wish to disclose.
- Designate the Recipient: List the individuals or organizations authorized to receive this information.
- Specify the Purpose: Detail the purpose for disclosure to ensure it aligns with your healthcare objectives.
- Sign and Date: Ensure the form is signed and dated by the beneficiary or their legal representative.
- Submit the Form: Return the completed form to Medicare as directed.
Why Use the CMS10106 1-800-MEDICARE Form
Using this form is essential for safeguarding personal health information while allowing necessary parties to access information critical for informed healthcare decisions. It empowers beneficiaries to control their health data, ensuring confidentiality and appropriate use.
Key Elements of the CMS10106 1-800-MEDICARE Form
- Beneficiary Information: Includes full name and Medicare Number.
- Details of Information to be Disclosed: Types of health information specified.
- Authorized Recipients: Designated individuals or entities.
- Purpose of Disclosure: Clearly stated reasons for the disclosure.
- Signature Requirement: Must be signed by the beneficiary or their representative.
Important Terms Related to the CMS10106 1-800-MEDICARE Form
- Authorization: Consent by the beneficiary for sharing specific information.
- Beneficiary: The individual covered under Medicare.
- Designated Party: The person or organization authorized to receive information.
- Confidentiality: Protection of personal health information from unauthorized access.
State-Specific Rules for the CMS10106 1-800-MEDICARE Form
Certain states, like New York, have unique requirements regarding the disclosure of sensitive health information. While the form generally allows for uniform application across states, beneficiaries should verify if state-specific guidelines affect their authorization, especially regarding mental health or substance abuse information.
Legal Use of the CMS10106 1-800-MEDICARE Form
The form complies with federal regulations ensuring the legal and secure handling of personal health information. It's designed to align with the Health Insurance Portability and Accountability Act (HIPAA), offering legal protection to beneficiaries by controlling access to their health data.
Examples of Using the CMS10106 1-800-MEDICARE Form
- Family Care Coordination: Authorizing a family member to discuss treatment plans with doctors.
- Healthcare Provider Communication: Enabling different medical specialists to share diagnosis information for comprehensive care.
- Long-term Care Facilities: Allowing nursing homes to access necessary medical records for resident care planning.
Form Submission Methods
Beneficiaries can submit the form online through Medicare's website, via mail, or in-person at Social Security offices. Online submission is often the fastest and most convenient method, while mail might be necessary for individuals without internet access.
Legal Use and Compliance
This form ensures compliance with privacy laws by requiring explicit consent for information disclosure. It's a critical legal tool for beneficiaries, reinforcing their rights to privacy and informed consent in healthcare.