01. Edit your united healthcare enrollment form 2024 online
Type text, add images, blackout confidential details, add comments, highlights and more.
02. Sign it in a few clicks
Draw your signature, type it, upload its image, or use your mobile device as a signature pad.
03. Share your form with others
Send united healthcare enrollment form via email, link, or fax. You can also download it, export it or print it out.
How to use or fill out employee enrollment form with our platform
Ease of Setup
DocHub User Ratings on G2
Ease of Use
DocHub User Ratings on G2
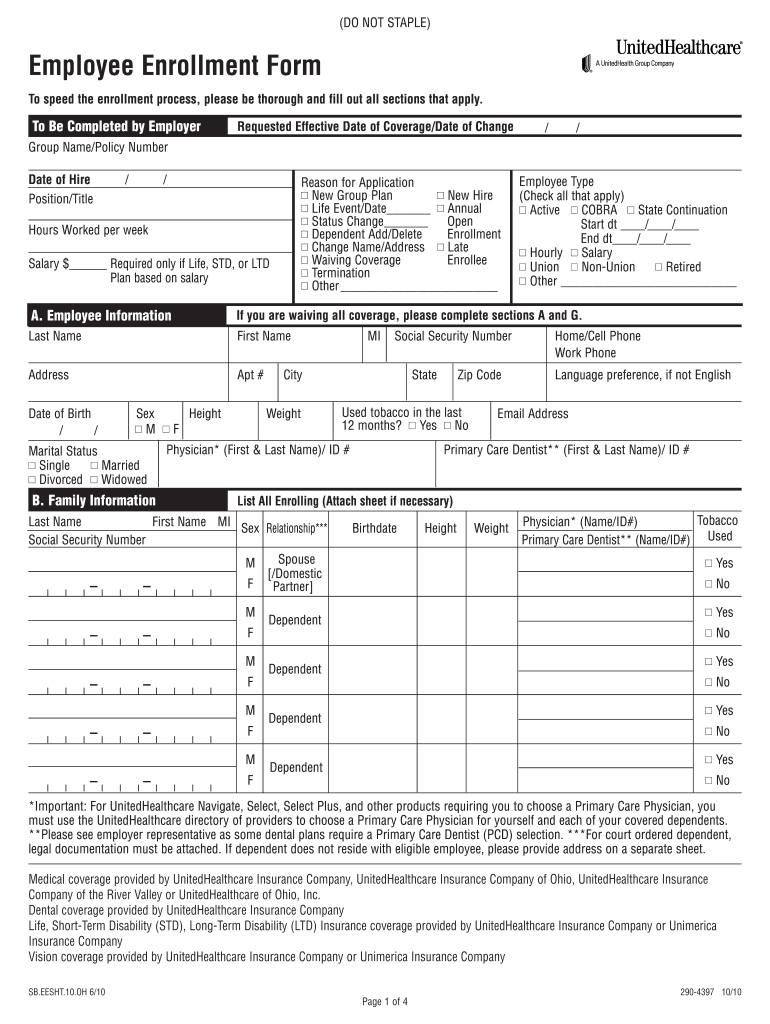
Click ‘Get Form’ to open the employee enrollment form in the editor.
Begin by filling out the 'Group' section, including your name, requested effective date of coverage, and group name or policy number.
In the 'Reason for Application' section, select the appropriate option that applies to your situation, such as 'New Hire' or 'Life Event'.
Complete Section A with your personal information: last name, first name, address, date of birth, sex, marital status, and contact details.
In Section B, list all enrolling dependents. Ensure you provide their names, relationships, and relevant health information.
Proceed to Section C to select your desired coverage options for medical, dental, and vision plans. Indicate any additional benefits you wish to enroll in.
Fill out Sections D and E regarding prior medical insurance information and other medical coverage details if applicable.
Finally, review all sections for accuracy before signing in Section H to authorize the submission of your application.
Start using our platform today for free to streamline your employee enrollment process!
Fill out employee enrollment form online It's free
Employee enrollment form templateEmployee enrollment form pdfFree employee enrollment formEmployee enrollment form template freeEmployee enrollment form onlineNew employee Forms I-9New employee forms w4United healthcare employee enrollment form 2025
Security and compliance
At DocHub, your data security is our priority. We follow HIPAA, SOC2, GDPR, and other standards, so you can work on your documents with confidence.
Health Benefits Plan Enrollment Form for Active Employees
I ELECT TO ENROLL in (or MAKE CHANGES TO) a health benefits plan as indicated above and agree to authorize deductions from (1) my salary to cover my share.Read more
Employee Enrollment Application / Change Request Form
Please complete this form in blue or black ink and submit to your employer when complete. Hours worked by employee per week. Date of hire (mm/dd/yyyy). LeftRead more
Cookie consent notice
This site uses cookies to enhance site navigation and personalize your experience.
By using this site you agree to our use of cookies as described in our Privacy Notice.
You can modify your selections by visiting our Cookie and Advertising Notice.