


Definition & Meaning
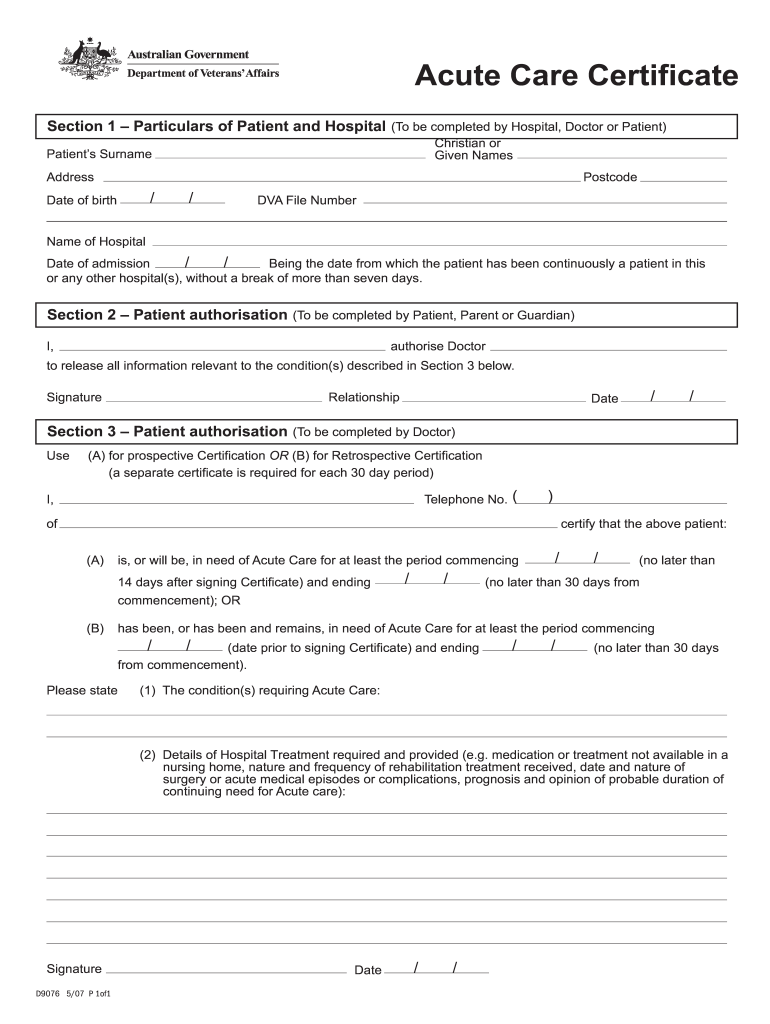
The "Section 1 Particulars of Patient and Hospital" is a crucial part of an Acute Care Certificate, serving as the foundational element for documenting patient and hospital details. This section is generally completed by the hospital staff, a doctor, or even the patient, depending on the procedural requirements and circumstances. Its primary purpose is to gather and verify critical patient information, such as name, age, and medical history, along with hospital details like the facility's name and location. This information is essential for the certification of the patient's need for acute care, ensuring that all required details for further medical action are thoroughly documented.
Key Elements of Section 1
This section involves several vital components, which collectively form a comprehensive profile of the patient and hospital:
- Patient Details: Typically includes full name, date of birth, address, and contact information to accurately identify the individual needing medical attention.
- Hospital Information: Captures the name of the hospital, its address, and contact numbers to ensure a clear understanding of where the patient will receive care.
- Medical Identification Numbers: Can include details like a patient ID or social security number, helping to link the patient to their medical records accurately.
Each piece of information should be filled out with precision to avoid any discrepancies during subsequent medical procedures or documentation processes.
Steps to Complete Section 1
Completing the Section 1 form involves a systematic step-by-step process to ensure thoroughness and accuracy:
- Gather Patient Information: Begin by collecting all necessary personal details of the patient from identity documents or prior medical records.
- Fill Hospital Details: Provide comprehensive information about the hospital where the patient is receiving or will receive care.
- Enter Medical Numbers: Include relevant identification numbers to streamline documentation and future data retrieval processes.
- Validate Information: Double-check each entry to ensure accuracy, comparing with legal documents or prior records available within the hospital system.
These steps are critical in maintaining the integrity and reliability of the document and ensuring legal compliance.
How to Use Section 1
Using this form effectively involves understanding its purpose within the broader context of medical record-keeping:
- Authorization and Consent: Consent may be required from the patient or their representative to release information.
- Data Collection and Verification: The form acts as a tool for consolidating patient and hospital details, facilitating smooth transitions in care and medical intervention.
- Documentation for Medical Procedures: This section provides the groundwork needed for any additional documentation, certifications, or patient care forms that the medical facility may require.
Why the Section is Important
The critical nature of Section 1 lies in its role in fostering precise communication among medical personnel involved in providing acute care. Documenting patient particulars enables:
- Accurate Diagnosis and Treatment: Facilitates informed decision-making based on a complete overview of patient information.
- Legal Compliance: Helps ensure that all documentation complies with statutory requirements, protecting both the patient and the medical institution.
- Efficient Care Coordination: Allows easy access to crucial data when coordinating multiple aspects of patient care, improving overall treatment efficiency.
Who Typically Uses This Form
Several stakeholders are involved in utilizing this form, each playing a pivotal role:
- Hospital Administration: Ensures that all patient data is correctly filed and organized.
- Healthcare Providers: Doctors and nurses use it to gather contextual patient information necessary for treatment plans.
- Patients or Guardians: May be directly involved if providing specific authorization or personal details not available through medical records.
Each party contributes to the accuracy and completeness of the form, crucial for the patient's treatment journey.
Important Terms Related to Section 1
Understanding the terminology used in the form enhances accurate completion and interpretation:
- Acute Care: A branch of secondary health care concerned with short-term treatment.
- Patient ID: A unique identifier assigned to a patient’s medical records for tracking purposes.
- Certification of Need: Document proving the necessity of medical intervention or care, often a part of this form.
Familiarity with these terms ensures that all parties involved in completing or reviewing the form can interpret the data correctly.
Legal Use of Section 1
There are specific legal considerations tied to the use of this form:
- Confidentiality and HIPAA Compliance: Patient information must be handled with care, adhering to medical confidentiality laws.
- Legal Verification: This form can act as a verified record should there be any legal examination of a patient's need for care.
- Documentation of Intent: An essential part of proving the intent and necessity of acute care provisioning, safeguarding both the healthcare provider and patient under potential disputes.
These legal aspects must be meticulously observed to uphold ethical and statutory medical practices.